

Epilepsy related to developmental tumors and malformations of cortical development
- PMID: 24481729
- PMCID: PMC3996119
- DOI: 10.1007/s13311-013-0251-0
Epilepsy related to developmental tumors and malformations of cortical development
Abstract
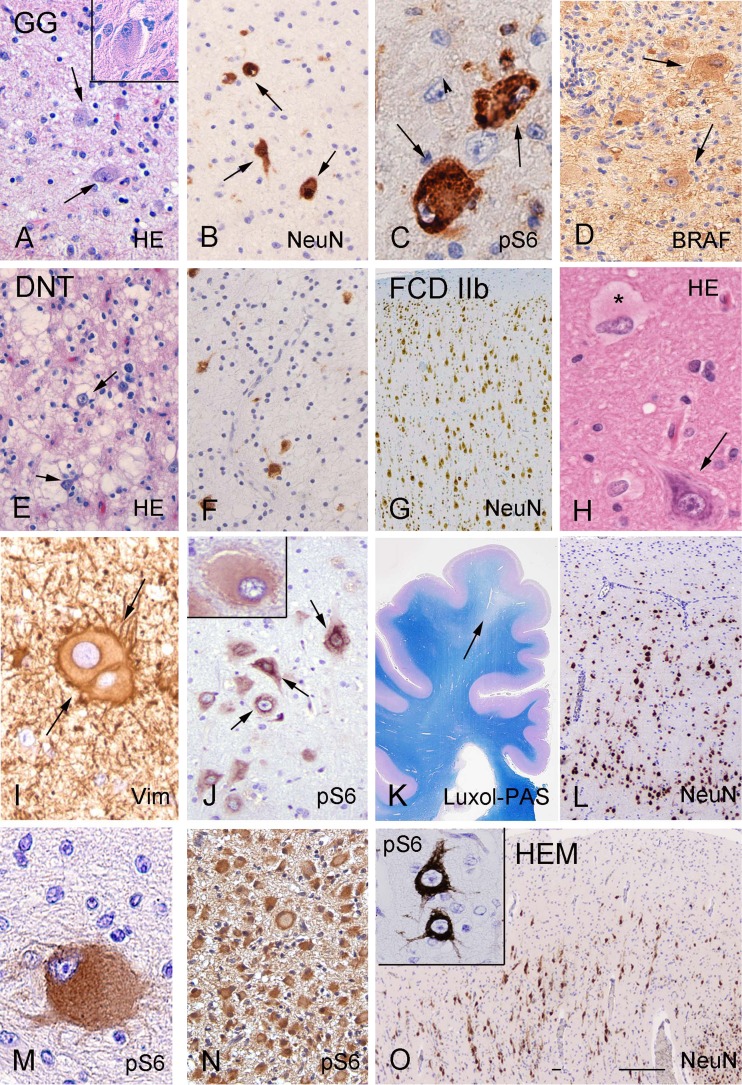
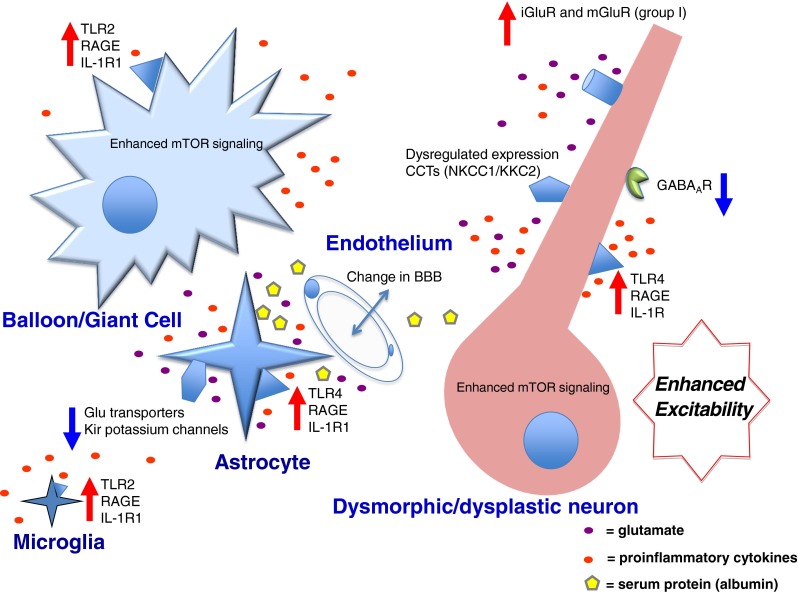
Structural abnormalities of the brain are increasingly recognized in patients with neurodevelopmental delay and intractable focal epilepsies. The access to clinically well-characterized neurosurgical material has provided a unique opportunity to better define the neuropathological, neurochemical, and molecular features of epilepsy-associated focal developmental lesions. These studies help to further understand the epileptogenic mechanisms of these lesions. Neuropathological evaluation of surgical specimens from patients with epilepsy-associated developmental lesions reveals two major pathologies: focal cortical dysplasia and low-grade developmental tumors (glioneuronal tumors). In the last few years there have been major advances in the recognition of a wide spectrum of developmental lesions associated with a intractable epilepsy, including cortical tubers in patients with tuberous sclerosis complex and hemimegalencephaly. As an increasing number of entities are identified, the development of a unified and comprehensive classification represents a great challenge and requires continuous updates. The present article reviews current knowledge of molecular pathogenesis and the pathophysiological mechanisms of epileptogenesis in this group of developmental disorders. Both emerging neuropathological and basic science evidence will be analyzed, highlighting the involvement of different, but often converging, pathogenetic and epileptogenic mechanisms, which may create the basis for new therapeutic strategies in these disorders.
Figures

References
-
- Blumcke I, Vinters HV, Armstrong D, Aronica E, Thom M, Spreafico R. Malformations of cortical development and epilepsies: neuropathological findings with emphasis on focal cortical dysplasia. Epileptic Disord. 2009;11:181–193. - PubMed
-
- Sisodiya SM, Fauser S, Cross JH, Thom M. Focal cortical dysplasia type II: biological features and clinical perspectives. Lancet Neurol. 2009;8:830–843. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
