

A metabolic biosignature of early response to anti-tuberculosis treatment
- PMID: 24484441
- PMCID: PMC3918231
- DOI: 10.1186/1471-2334-14-53
A metabolic biosignature of early response to anti-tuberculosis treatment
Abstract
Background: The successful treatment of tuberculosis (TB) requires long-term multidrug chemotherapy. Clinical trials to evaluate new drugs and regimens for TB treatment are protracted due to the slow clearance of Mycobacterium tuberculosis (Mtb) infection and the lack of early biomarkers to predict treatment outcome. Advancements in the field of metabolomics make it possible to identify metabolic profiles that correlate with disease states or successful chemotherapy. However, proof-of-concept of this approach has not been provided for a TB-early treatment response biosignature (TB-ETRB).
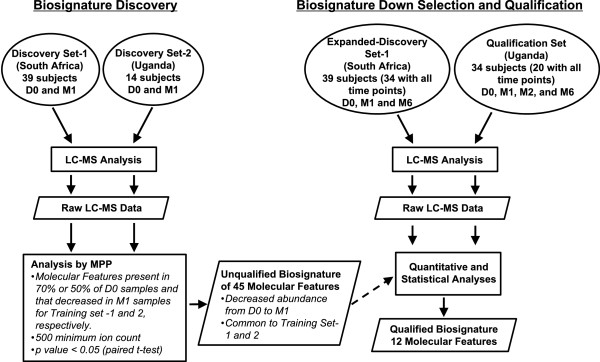
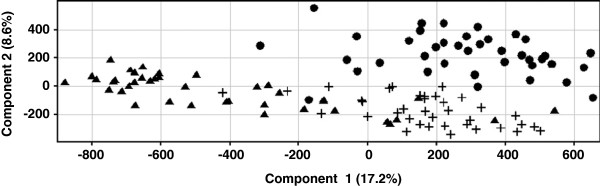
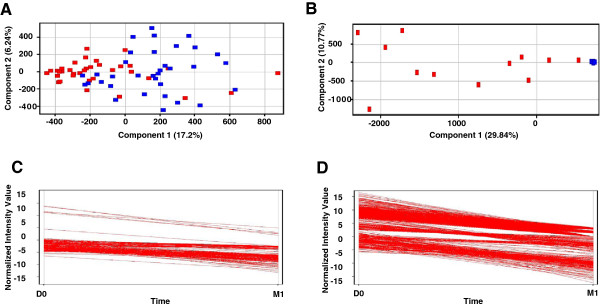
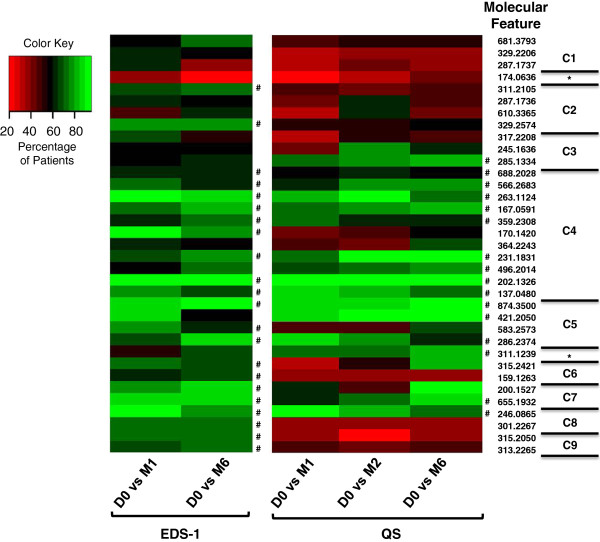
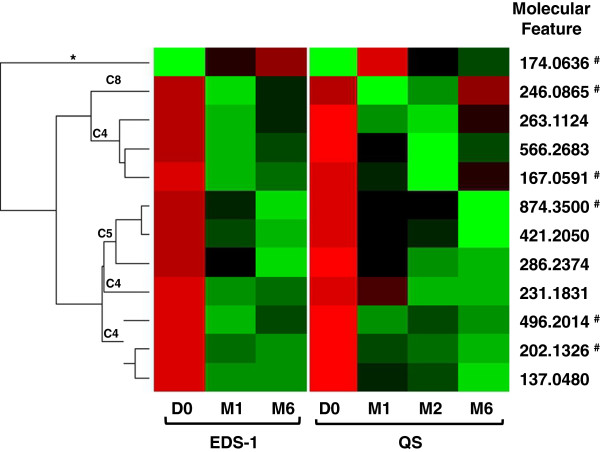
Methods: Urine samples collected at baseline and during treatment from 48 Ugandan and 39 South African HIV-seronegative adults with pulmonary TB were divided into discovery and qualification sets, normalized to creatinine concentration, and analyzed by liquid chromatography-mass spectrometry to identify small molecule molecular features (MFs) in individual patient samples. A biosignature that distinguished baseline and 1 month treatment samples was selected by pairwise t-test using data from two discovery sample sets. Hierarchical clustering and repeated measures analysis were applied to additional sample data to down select molecular features that behaved consistently between the two clinical sites and these were evaluated by logistic regression analysis.
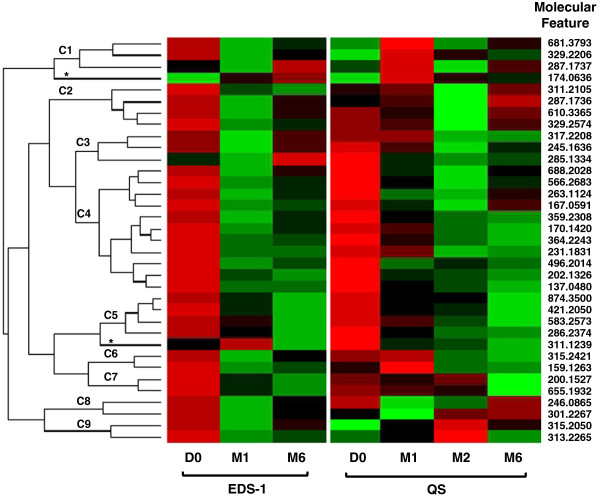
Results: Analysis of discovery samples identified 45 MFs that significantly changed in abundance at one month of treatment. Down selection using an extended set of discovery samples and qualification samples confirmed 23 MFs that consistently changed in abundance between baseline and 1, 2 and 6 months of therapy, with 12 MFs achieving statistical significance (p < 0.05). Six MFs classified the baseline and 1 month samples with an error rate of 11.8%.
Conclusions: These results define a urine based TB-early treatment response biosignature (TB-ETRB) applicable to different parts of Africa, and provide proof-of-concept for further evaluation of this technology in monitoring clinical responses to TB therapy.
Figures
References
-
- Nahid P, Saukkonen J, Mac Kenzie WR, Johnson JL, Phillips PP, Andersen J, Bliven-Sizemore E, Belisle JT, Boom WH, Luetkemeyer A. et al. CDC/NIH workshop. Tuberculosis biomarker and surrogate endpoint research roadmap. Am J Respir Crit Care Med. 2011;14(8):972–979. doi: 10.1164/rccm.201105-0827WS. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
