

Maternal morbidity and preterm birth in 22 low- and middle-income countries: a secondary analysis of the WHO Global Survey dataset
- PMID: 24484741
- PMCID: PMC3913333
- DOI: 10.1186/1471-2393-14-56
Maternal morbidity and preterm birth in 22 low- and middle-income countries: a secondary analysis of the WHO Global Survey dataset
Abstract
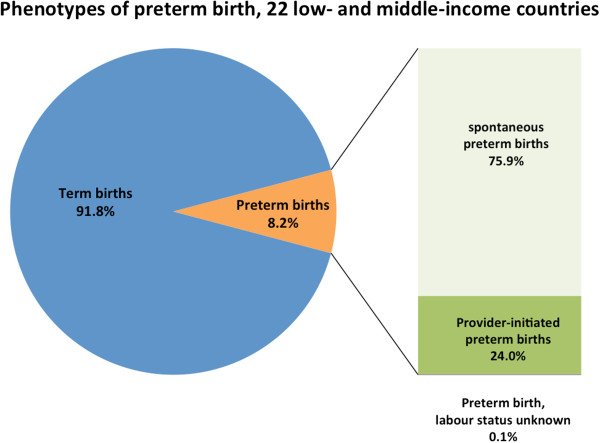
Background: Preterm birth (PTB) (<37weeks) complicates approximately 15 million deliveries annually, 60% occurring in low- and middle-income countries (LMICs). Several maternal morbidities increase the risk of spontaneous (spPTB) and provider-initiated (piPTB) preterm birth, but there is little data from LMICs.
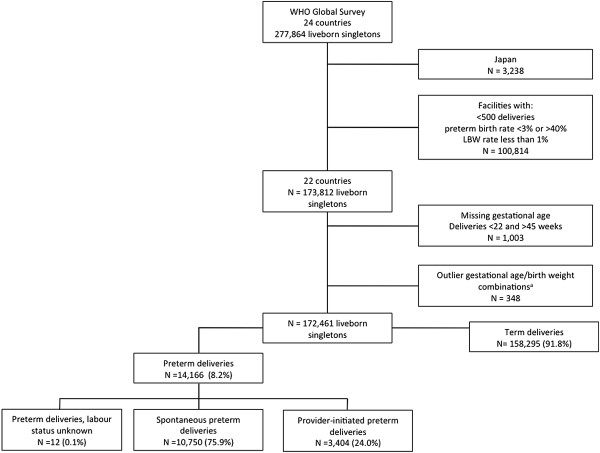
Method: We used the WHO Global Survey to analyze data from 172,461 singleton deliveries in 145 facilities across 22 LMICs. PTB and six maternal morbidities (height <145 cm, malaria, HIV/AIDS, pyelonephritis/UTI, diabetes and pre-eclampsia) were investigated. We described associated characteristics and developed multilevel models for the risk of spPTB/piPTB associated with maternal morbidities. Adverse perinatal outcomes (Apgar <7 at 5 minutes, NICU admission, stillbirth, early neonatal death and low birthweight) were determined.
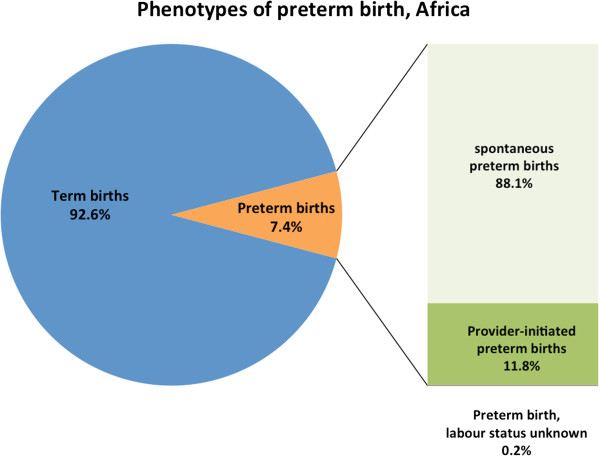
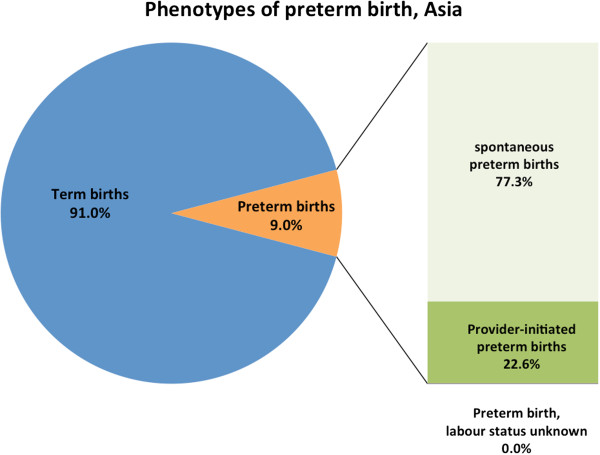
Results: 8.2% of deliveries were PTB; one-quarter of these were piPTB. 14.2% of piPTBs were not medically indicated. Maternal height <145 cm (AOR 1.30, 95% CI 1.10-1.52), pyelonephritis/UTI (AOR 1.16, 95% CI 1.01-1.33), pre-gestational diabetes (AOR 1.41, 95% CI 1.09-1.82) and pre-eclampsia (AOR 1.25, 95% CI 1.05-1.49) increased odds of spPTB, as did malaria in Africa (AOR 1.67, 95%CI 1.32-2.11) but not HIV/AIDS (AOR 1.17, 95% CI 0.79-1.73). Odds of piPTB were higher with maternal height <145 cm (AOR 1.47, 95% CI 1.23-1.77), pre-gestational diabetes (AOR 2.51, 95% CI 1.81-3.47) and pre-eclampsia (AOR 8.17, 95% CI 6.80-9.83).
Conclusions: Maternal height <145 cm, diabetes and pre-eclampsia significantly increased odds of spPTB and piPTB, while pyelonephritis/UTI and malaria increased odds of spPTB only. Strategies to reduce PTB and associated newborn morbidity/mortality in LMICs must prioritize antenatal screening/treatment of these common conditions and reducing non-medically indicated piPTBs where appropriate.
Figures



References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, Adler A, Garcia CV, Rohde S, Say L, Lawn JE. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–2172. doi: 10.1016/S0140-6736(12)60820-4. - DOI - PubMed
-
- Teune MJ, Bakhuizen S, Bannerman CG. A systematic review of severe morbidity in infants born late preterm. AJOG. 2011;205:374. - PubMed
-
- Katz J, Lee AC, Kozuki N, Lawn JE, Blencowe H, Ezzati M. CHERG Preterm-SGA Working Group. Born too small or too soon: a pooled analysis of mortality risk among preterm and small-for-gestational-age infants in low- and middle-income countries. Lancet. 2013;382(9890):417–425. doi: 10.1016/S0140-6736(13)60993-9. - DOI - PMC - PubMed
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, Rudan I, Campbell H, Cibulskis R, Li M, Mathers C, Black RE. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–2161. doi: 10.1016/S0140-6736(12)60560-1. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
