

Exploring necrotizing autoimmune myopathies with a novel immunoassay for anti-3-hydroxy-3-methyl-glutaryl-CoA reductase autoantibodies
- PMID: 24484965
- PMCID: PMC3979083
- DOI: 10.1186/ar4468
Exploring necrotizing autoimmune myopathies with a novel immunoassay for anti-3-hydroxy-3-methyl-glutaryl-CoA reductase autoantibodies
Abstract
Introduction: Necrotizing autoimmune myopathies (NAM) have recently been defined as a distinct group of severe acquired myopathies, characterized by prominent myofiber necrosis without significant muscle inflammation. Because of the lack of appropriate biomarkers, these diseases have been long misdiagnosed as atypical forms of myositis. NAM may be associated to autoantibodies directed against signal recognition particle (SRP) or 3-hydroxy-3-methyl-glutaryl-CoA reductase (HMGCR). The objective of this work was to quantify anti-HMGCR autoantibodies in patients with suspicion of NAM through the development of a new addressable laser bead immunoassay (ALBIA).
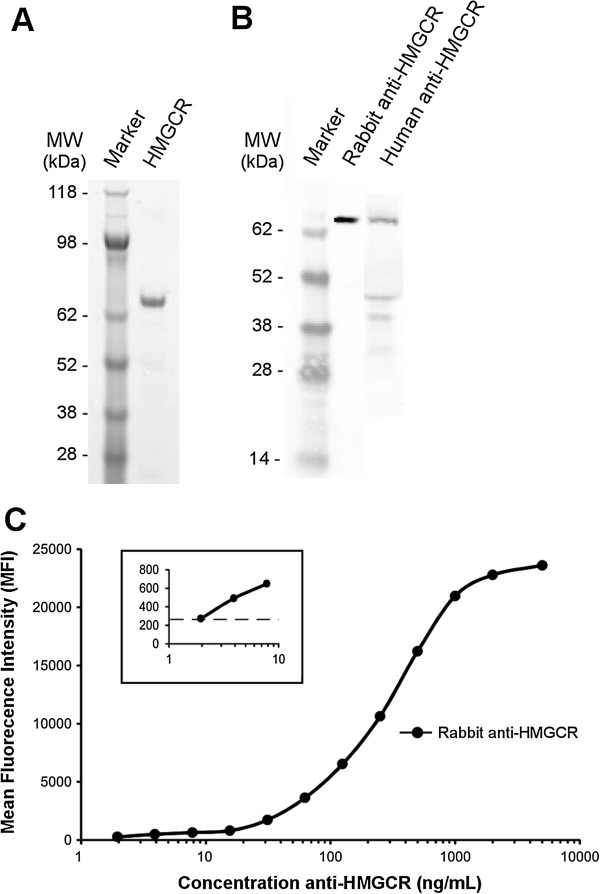
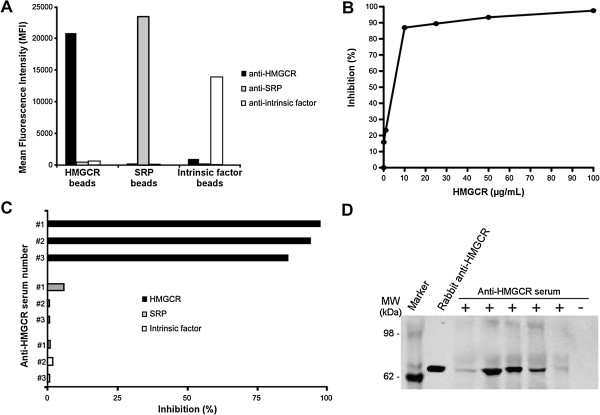
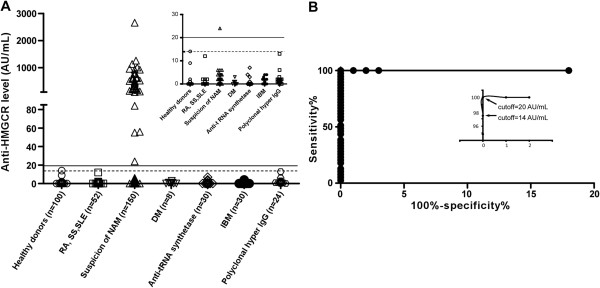
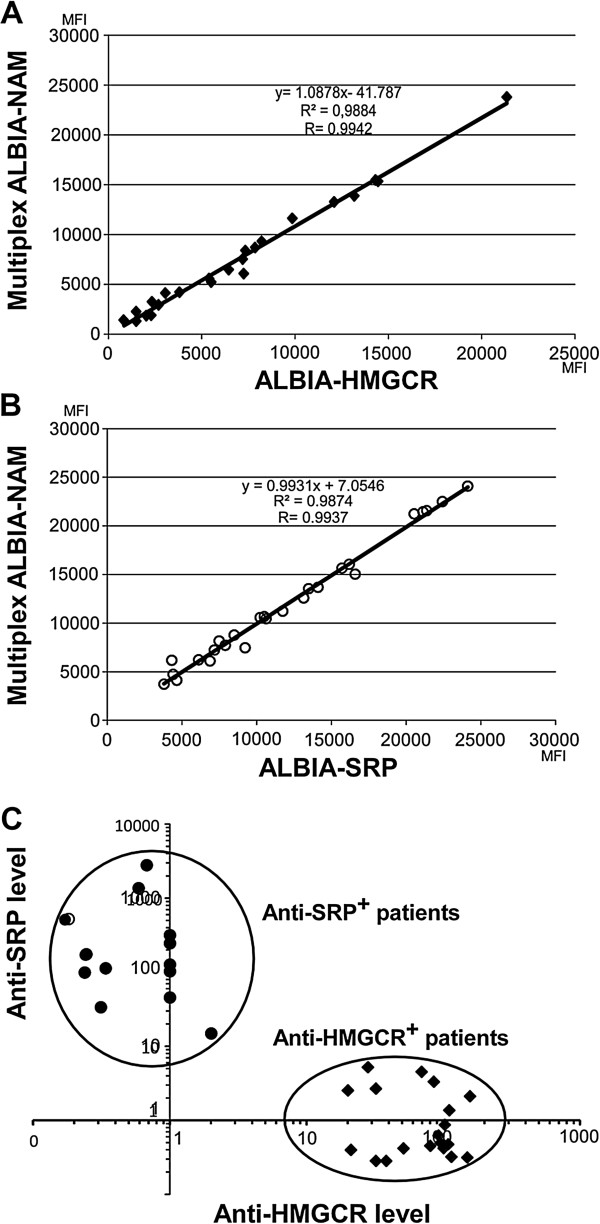
Methods: Recombinant HMGCR C-domain was bound to fluorescent beads. After incubation with serum, autoantibodies were revealed using class- or subclass-specific anti-human immunoglobulin G (IgG) antibodies. Anti-HMGCR levels were assayed in 150 patients with suspicion of NAM, 142 controls with different inflammatory/autoimmune diseases and 100 healthy donors. Inhibition with free recombinant HMGCR and immunoprecipitation experiments confirmed test specificity. Reproducibility and repeatability were determined from sera with various levels of anti-HMGCR autoantibodies. A multiplex assay (ALBIA-NAM) was also developed to permit the simultaneous quantification of anti-HMGCR and anti-signal recognition particle autoantibodies.
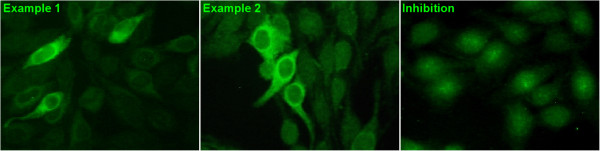
Results: No controls scored positive. Of 150 patients with suspicion of NAM, 24% were positive for anti-HMGCR autoantibodies with levels ranging from 24 to 2,656 AU/mL. Anti-HMGCR positivity could be associated to a cytoplasmic pattern in immunofluorescence assay on HEp-2 cells. Anti-HMGCR-positive patients had high creatine kinase (CK) levels (mean 6,630 IU/L) and only 40% of them had been exposed to statins. Multiplex ALBIA-NAM was equally as effective as monoplex anti-HMGCR and anti-SRP ALBIA.
Conclusions: Both monoplex ALBIA-HMGCR and multiplex ALBIA-NAM reliably detect and quantify anti-HMGCR autoantibodies. A positive result allows ascribing patients with a necrotizing myopathy to an autoimmune form. Anti-HMGCR autoantibodies may be found in patients who have not taken statins.
Figures
Comment in
-
Exploring necrotizing autoimmune myopathies with a novel immunoassay for anti-3-hydroxy-3-methyl-glutaryl-CoA reductase autoantibodies.Ann Clin Biochem. 2014 Jul;51(4):516. doi: 10.1177/0004563214538903. Ann Clin Biochem. 2014. PMID: 28071082 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
