

Prevention and treatment of acute radiation-induced skin reactions: a systematic review and meta-analysis of randomized controlled trials
- PMID: 24484999
- PMCID: PMC3909507
- DOI: 10.1186/1471-2407-14-53
Prevention and treatment of acute radiation-induced skin reactions: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Radiation-induced skin reaction (RISR) is a common side effect that affects the majority of cancer patients receiving radiation treatment. RISR is often characterised by swelling, redness, pigmentation, fibrosis, and ulceration, pain, warmth, burning, and itching of the skin. The aim of this systematic review was to assess the effects of interventions which aim to prevent or manage RISR in people with cancer.
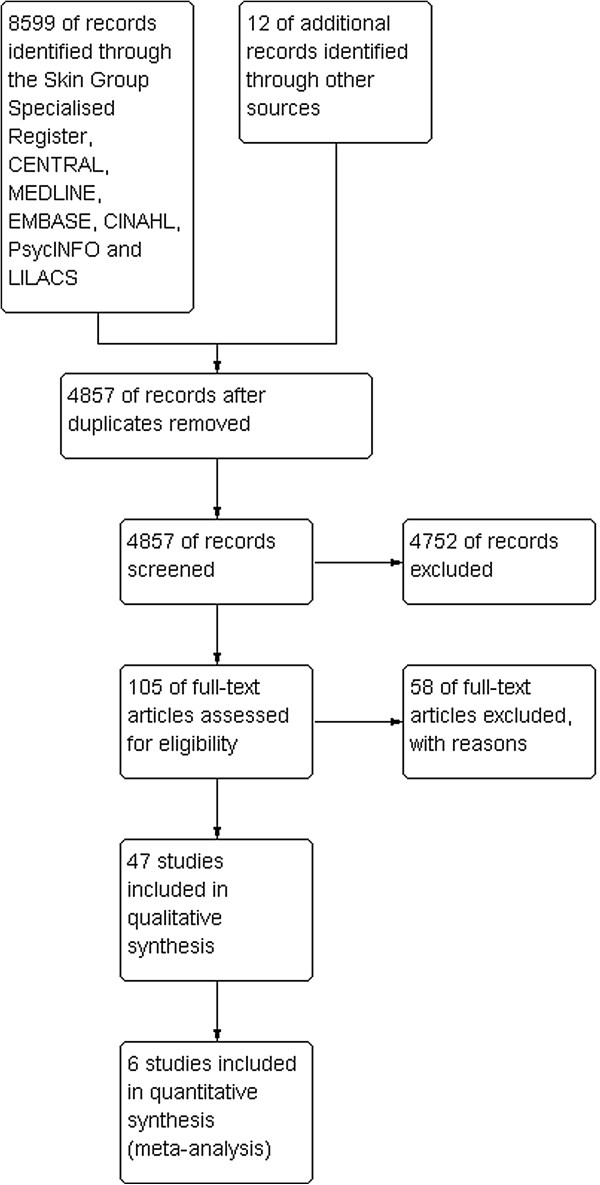
Methods: We searched the following databases up to November 2012: Cochrane Skin Group Specialised Register, CENTRAL (2012, Issue 11), MEDLINE (from 1946), EMBASE (from 1974), PsycINFO (from 1806), CINAHL (from 1981) and LILACS (from 1982). Randomized controlled trials evaluating interventions for preventing or managing RISR in cancer patients were included. The primary outcomes were development of RISR, and levels of RISR and symptom severity. Secondary outcomes were time taken to develop erythema or dry desquamation; quality of life; time taken to heal, a number of skin reaction and symptom severity measures; cost, participant satisfaction; ease of use and adverse effects. Where appropriate, we pooled results of randomized controlled trials using mean differences (MD) or odd ratios (OR) with 95% confidence intervals (CI).
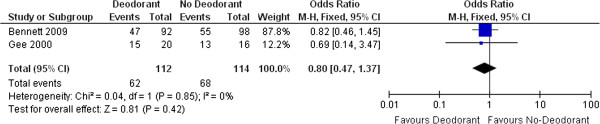
Results: Forty-seven studies were included in this review. These evaluated six types of interventions (oral systemic medications; skin care practices; steroidal topical therapies; non-steroidal topical therapies; dressings and other). Findings from two meta-analyses demonstrated significant benefits of oral Wobe-Mugos E for preventing RISR (OR 0.13 (95% CI 0.05 to 0.38)) and limiting the maximal level of RISR (MD -0.92 (95% CI -1.36 to -0.48)). Another meta-analysis reported that wearing deodorant does not influence the development of RISR (OR 0.80 (95% CI 0.47 to 1.37)).
Conclusions: Despite the high number of trials in this area, there is limited good, comparative research that provides definitive results suggesting the effectiveness of any single intervention for reducing RISR. More research is required to demonstrate the usefulness of a wide range of products that are being used for reducing RISR. Future efforts for reducing RISR severity should focus on promising interventions, such as Wobe-Mugos E and oral zinc.
Figures



References
-
- Sitton E. Early and late radiation-induced skin alterations. Part II: Nursing care of irradiated skin. Oncol Nurs Forum. 1992;19(6):907–912. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
