

Clinical disease activity and acute phase reactant levels are discordant among patients with active rheumatoid arthritis: acute phase reactant levels contribute separately to predicting outcome at one year
- PMID: 24485007
- PMCID: PMC3978994
- DOI: 10.1186/ar4469
Clinical disease activity and acute phase reactant levels are discordant among patients with active rheumatoid arthritis: acute phase reactant levels contribute separately to predicting outcome at one year
Abstract
Introduction: Clinical trials of new treatments for rheumatoid arthritis (RA) typically require subjects to have an elevated acute phase reactant (APR), in addition to tender and swollen joints. However, despite the elevation of individual components of the Clinical Disease Activity Index (CDAI) (tender and swollen joint counts and patient and physician global assessment), some patients with active RA may have normal erythrocyte sedimentation rate (ESR) and/or C-reactive protein (CRP) levels and thus fail to meet entry criteria for clinical trials. We assessed the relationship between CDAI and APRs in the Consortium of Rheumatology Researchers of North America (CORRONA) registry by comparing baseline characteristics and one-year clinical outcomes of patients with active RA, grouped by baseline APR levels.
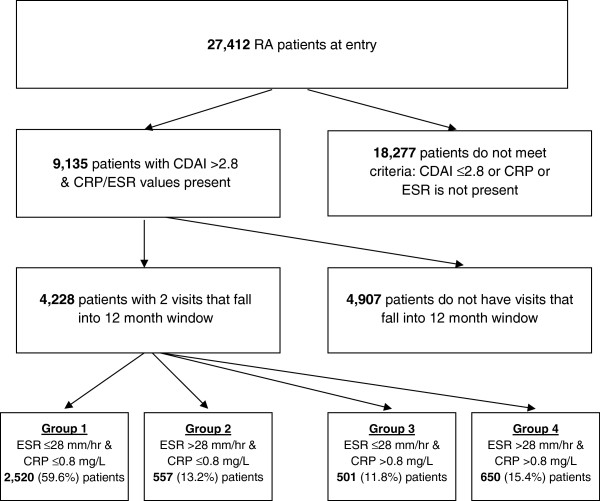
Methods: This was an observational study of 9,135 RA patients who had both ESR and CRP drawn and a visit at which CDAI was >2.8 (not in remission).
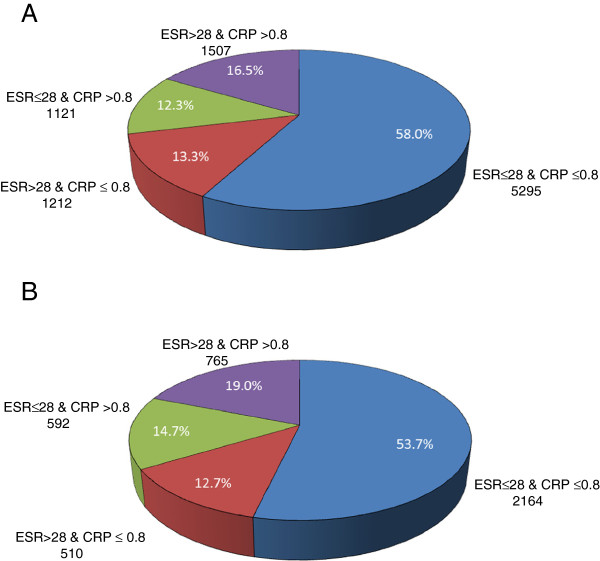
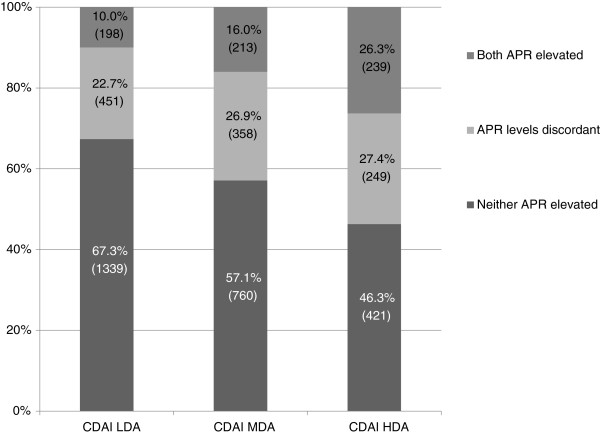
Results: Of 9,135 patients with active RA, 58% had neither elevated ESR nor CRP; only 16% had both elevated ESR and CRP and 26% had either ESR or CRP elevated. Among the 4,228 patients who had a one-year follow-up visit, both baseline and one-year follow-up modified Health Assessment Questionnaire (mHAQ) and CDAI scores were lowest for patients with active RA but with neither APR elevated; both mHAQ and CDAI scores increased sequentially with the increase in number of elevated APR levels at baseline. Each individual component of the CDAI followed the same trend, both at baseline and at one-year follow-up. The magnitude of improvement in both CDAI and mHAQ scores at one year was associated positively with the number of APRs elevated at baseline.
Conclusions: In a large United States registry of RA patients, APR levels often do not correlate with disease activity as measured by joint counts and global assessments. These data strongly suggest that it is appropriate to obtain both ESR and CRP from RA patients at the initial visit. Requiring an elevation in APR levels as a criterion for inclusion of RA patients in studies of experimental agents may exclude some patients with active disease.
Figures
Similar articles
-
Clinical outcomes of patients with active rheumatoid arthritis with normal acute phase reactant values.Int J Rheum Dis. 2019 May;22(5):852-859. doi: 10.1111/1756-185X.13469. Epub 2019 Jan 24. Int J Rheum Dis. 2019. PMID: 30677239
-
Which measure of inflammation to use? A comparison of erythrocyte sedimentation rate and C-reactive protein measurements from randomized clinical trials of golimumab in rheumatoid arthritis.J Rheumatol. 2009 Aug;36(8):1606-10. doi: 10.3899/jrheum.081188. Epub 2009 Jun 16. J Rheumatol. 2009. PMID: 19531760
-
Functional improvement after patients with rheumatoid arthritis start a new disease modifying antirheumatic drug (DMARD) associated with frequent changes in DMARD: the CORRONA database.J Rheumatol. 2008 Oct;35(10):1966-71. Epub 2008 Sep 1. J Rheumatol. 2008. PMID: 18785317 Free PMC article.
-
American College of Rheumatology/European League against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials.Ann Rheum Dis. 2011 Mar;70(3):404-13. doi: 10.1136/ard.2011.149765. Ann Rheum Dis. 2011. PMID: 21292833
-
American College of Rheumatology/European League Against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials.Arthritis Rheum. 2011 Mar;63(3):573-86. doi: 10.1002/art.30129. Arthritis Rheum. 2011. PMID: 21294106 Free PMC article.
Cited by
-
Comparison of remission criteria in patients with rheumatoid arthritis treated with biologic or targeted synthetic disease-modifying anti-rheumatic drugs: results from a nationwide registry.Ther Adv Musculoskelet Dis. 2022 May 13;14:1759720X221096363. doi: 10.1177/1759720X221096363. eCollection 2022. Ther Adv Musculoskelet Dis. 2022. PMID: 35586514 Free PMC article.
-
The relationship between serum C-reactive protein and senile hypertension.BMC Cardiovasc Disord. 2022 Nov 24;22(1):500. doi: 10.1186/s12872-022-02948-4. BMC Cardiovasc Disord. 2022. PMID: 36418968 Free PMC article.
-
Characterization of a Subset of Patients With Rheumatoid Arthritis for Whom Current Management Strategies are Inadequate.ACR Open Rheumatol. 2019 Apr 22;1(3):145-155. doi: 10.1002/acr2.1021. eCollection 2019 May. ACR Open Rheumatol. 2019. PMID: 31777790 Free PMC article.
-
Multibiomarker disease activity score and C-reactive protein in a cross-sectional observational study of patients with rheumatoid arthritis with and without concomitant fibromyalgia.Rheumatology (Oxford). 2016 Apr;55(4):640-8. doi: 10.1093/rheumatology/kev388. Epub 2015 Nov 25. Rheumatology (Oxford). 2016. PMID: 26608972 Free PMC article.
-
[Biomarkers for chronic inflammatory diseases].Z Rheumatol. 2015 Dec;74(10):887-96; quiz 897. doi: 10.1007/s00393-015-0009-7. Z Rheumatol. 2015. PMID: 26608264 Review. German.
References
-
- Dixey J, Solymossy C, Young A, Early RAS. Is it possible to predict radiological damage in early rheumatoid arthritis (RA)? A report on the occurrence, progression, and prognostic factors of radiological erosions over the first 3 years in 866 patients from the Early RA Study (ERAS) J Rheumatol Suppl. 2004;16:48–54. - PubMed
-
- Caruso I, Santandrea S, Sarzi Puttini P, Boccassini L, Montrone F, Cazzola M, Azzolini V, Segre D. Clinical, laboratory and radiographic features in early rheumatoid arthritis. J Rheumatol. 1990;16:1263–1267. - PubMed
-
- Wolfe F, Hawley DJ. The longterm outcomes of rheumatoid arthritis: Work disability: a prospective 18 year study of 823 patients. J Rheumatol. 1998;16:2108–2117. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
