

Pharmacologic regimens for knee osteoarthritis prevention: can they be cost-effective?
- PMID: 24487044
- PMCID: PMC4006219
- DOI: 10.1016/j.joca.2014.01.005
Pharmacologic regimens for knee osteoarthritis prevention: can they be cost-effective?
Abstract
Objective: We sought to determine the target populations and drug efficacy, toxicity, cost, and initiation age thresholds under which a pharmacologic regimen for knee osteoarthritis (OA) prevention could be cost-effective.
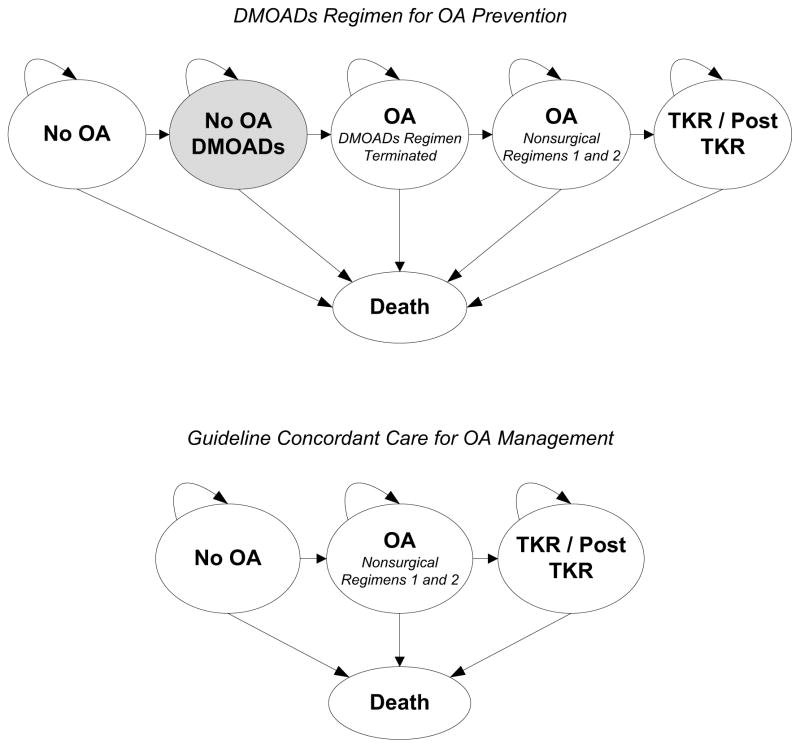
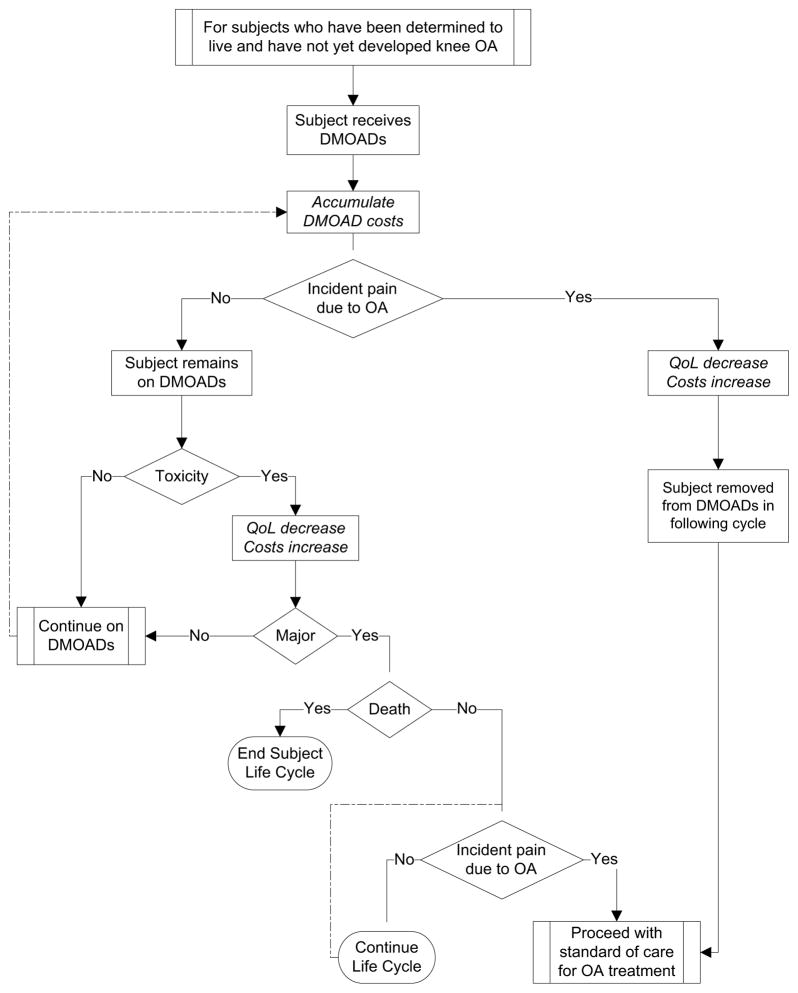
Design: We used the Osteoarthritis Policy (OAPol) Model, a validated state-transition simulation model of knee OA, to evaluate the cost-effectiveness of using disease-modifying OA drugs (DMOADs) as prophylaxis for the disease. We assessed four cohorts at varying risk for developing OA: (1) no risk factors, (2) obese, (3) history of knee injury, and (4) high-risk (obese with history of knee injury). The base case DMOAD was initiated at age 50 with 40% efficacy in the first year, 5% failure per subsequent year, 0.22% major toxicity, and annual cost of $1,000. Outcomes included costs, quality-adjusted life expectancy (QALE), and incremental cost-effectiveness ratios (ICERs). Key parameters were varied in sensitivity analyses.
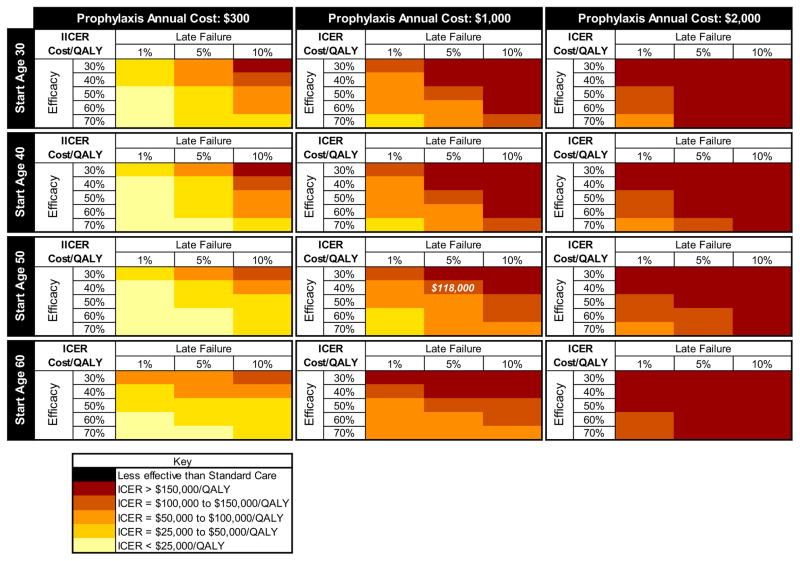
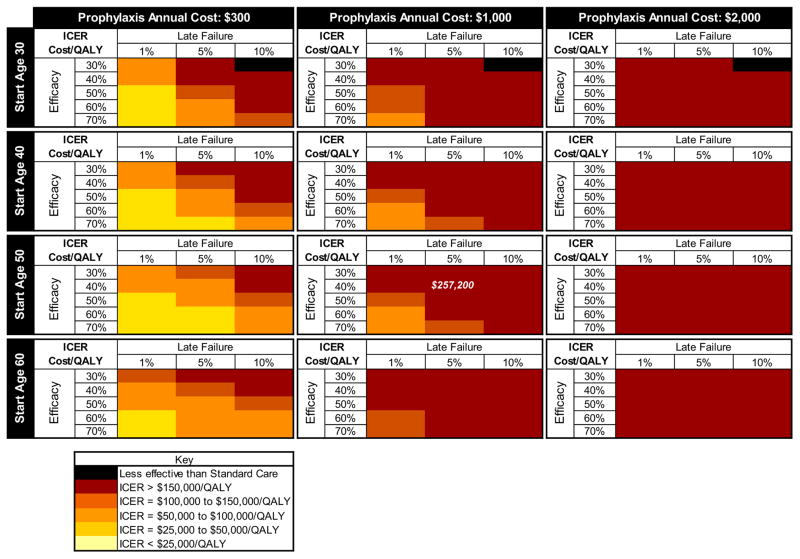
Results: For the high-risk cohort, base case prophylaxis increased quality-adjusted life-years (QALYs) by 0.04 and lifetime costs by $4,600, and produced an ICER of $118,000 per QALY gained. ICERs >$150,000/QALY were observed when comparing the base case DMOAD to the standard of care in the knee injury only cohort; for the obese only and no risk factors cohorts, the base case DMOAD was less cost-effective than the standard of care. Regimens priced at $3,000 per year and higher demonstrated ICERs above cost-effectiveness thresholds consistent with current US standards.
Conclusions: The cost-effectiveness of DMOADs for OA prevention for persons at high risk for incident OA may be comparable to other accepted preventive therapies.
Keywords: Cost-effectiveness; Disease-modifying osteoarthritis drugs; Knee osteoarthritis; Prophylaxis.
Copyright © 2014 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors do not have any conflict of interest with respect to the content of this paper.
Figures
References
-
- Losina E, Niu NN, Holt HL, Reichmann WM, Hunter DJ, Suter LG, et al. Cost-Effectiveness of ACR Guideline-Based Care and Lifetime Direct Medical Costs Attributable to Knee OA Management in the US. American College of Rheumatology (ACR) Annual Scientific Meeting; Philadelphia, PA: Arthritis & Rheumatism; 2009. p. 1177.
-
- Bitton R. The economic burden of osteoarthritis. Am J Manag Care. 2009;15:S230–235. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
