

Hospital variation in survival after in-hospital cardiac arrest
- PMID: 24487717
- PMCID: PMC3959682
- DOI: 10.1161/JAHA.113.000400
Hospital variation in survival after in-hospital cardiac arrest
Abstract
Background: In-hospital cardiac arrest (IHCA) is common and often fatal. However, the extent to which hospitals vary in survival outcomes and the degree to which this variation is explained by patient and hospital factors is unknown.
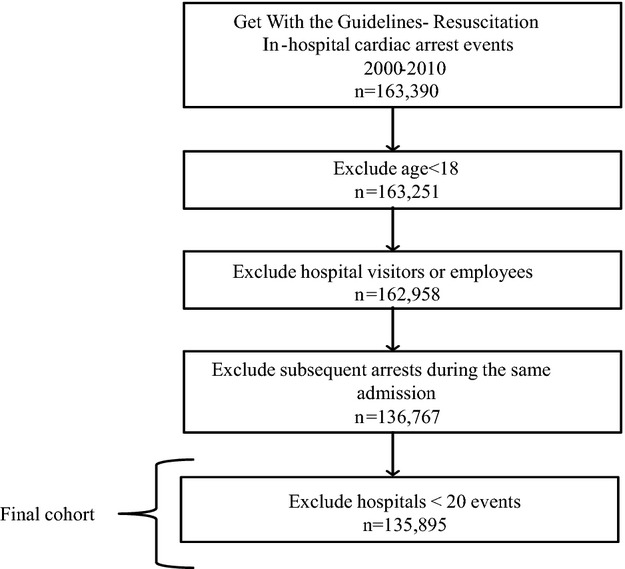
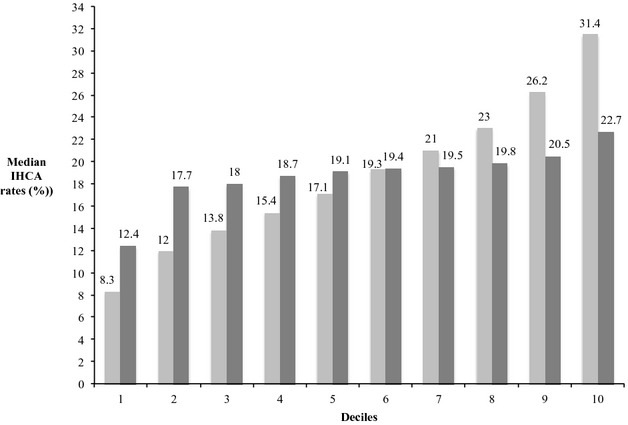
Methods and results: Within Get with the Guidelines-Resuscitation, we identified 135 896 index IHCA events at 468 hospitals. Using hierarchical models, we adjusted for demographics comorbidities and arrest characteristics (eg, initial rhythm, etiology, arrest location) to generate risk-adjusted rates of in-hospital survival. To quantify the extent of hospital-level variation in risk-adjusted rates, we calculated the median odds ratio (OR). Among study hospitals, there was significant variation in unadjusted survival rates. The median unadjusted rate for the bottom decile was 8.3% (range: 0% to 10.7%) and for the top decile was 31.4% (28.6% to 51.7%). After adjusting for 36 predictors of in-hospital survival, there remained substantial variation in rates of in-hospital survival across sites: bottom decile (median rate, 12.4% [0% to 15.6%]) versus top decile (median rate, 22.7% [21.0% to 36.2%]). The median OR for risk-adjusted survival was 1.42 (95% CI: 1.37 to 1.46), which suggests a substantial 42% difference in the odds of survival for patients with similar case-mix at similar hospitals. Further, significant variation persisted within hospital subgroups (eg, bed size, academic).
Conclusion: Significant variability in IHCA survival exists across hospitals, and this variation persists despite adjustment for measured patient factors and within hospital subgroups. These findings suggest that other hospital factors may account for the observed site-level variations in IHCA survival.
Keywords: cardiac arrest; cardiopulmonary resuscitation; heart arrest; resuscitation.
Figures
Comment in
-
Survival by the fittest: hospital-level variation in quality of resuscitation care.J Am Heart Assoc. 2014 Feb 28;3(1):e000768. doi: 10.1161/JAHA.113.000768. J Am Heart Assoc. 2014. PMID: 24584744 Free PMC article. No abstract available.
References
-
- Sandroni C, Nolan J, Cavallaro F, Antonelli M. In‐hospital cardiac arrest: incidence, prognosis and possible measures to improve survival. Intensive Care Med. 2007; 33:237-245 - PubMed
-
- Gwinnutt CL, Columb M, Harris R. Outcome after cardiac arrest in adults in UK hospitals: effect of the 1997 guidelines. Resuscitation. 2000; 47:125-135 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
