

Review
doi: 10.1038/nrmicro3200.
Epub 2014 Feb 3.
The path of anti-tuberculosis drugs: from blood to lesions to mycobacterial cells
Affiliations
- PMID: 24487820
- PMCID: PMC4341982
- DOI: 10.1038/nrmicro3200
Item in Clipboard
Review
The path of anti-tuberculosis drugs: from blood to lesions to mycobacterial cells
Nat Rev Microbiol.
2014 Mar.
Abstract
For the successful treatment of pulmonary tuberculosis, drugs need to penetrate complex lung lesions and permeate the mycobacterial cell wall in order to reach their intracellular targets. However, most currently used anti-tuberculosis drugs were introduced into clinical use without considering the pharmacokinetic and pharmacodynamic properties that influence drug distribution, and this has contributed to the long duration and limited success of current therapies. In this Progress article, I describe new methods to quantify and image drug distribution in infected lung tissue and in mycobacterial cells, and I explore how this technology could be used to design optimized multidrug regimens.
Figures
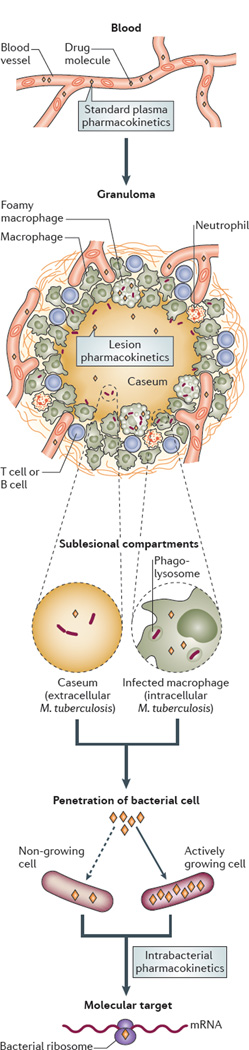
To reach their targets in intracellular bacilli, anti tuberculosis drugs travel from blood vessels and distribute into various types of lesions, and they must overcome several barriers, including variations in lesion architecture and the cellular and chemical composition of tissues, as well as reduced vascularization. From the blood compartment, drugs enter the interstitial space of granulomas and then penetrate and accumulate in immune cells, including within subcellular organelles, such as the phagolysosome, where intracellular bacilli can reside; finally, the drugs permeate the pathogen to reach their molecular target. In necrotic granulomas and cavities, drugs must diffuse through caseum in the absence of vascularization and active transport systems to reach extracellular bacilli that are present in the necrotic centre. Different lesion compartments can harbour bacterial populations in different metabolic and physiological states (for example, slowly-replicating or non-replicating bacilli), which can result in alterations in bacterial cell wall structure and transport mechanisms, which also influence the permeability of the pathogen to small drug molecules. Some drugs show reduced penetration of non-growing cells (dashed arrow) compared to growing cells, whereas others effectively penetrate both cell types (not shown).
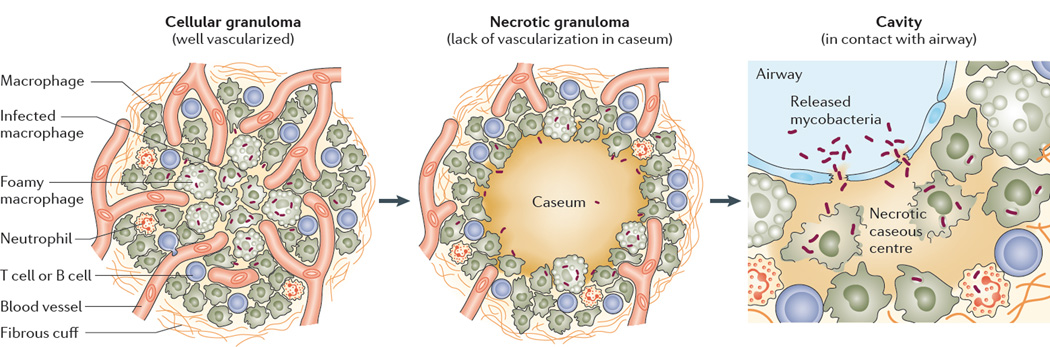
The granuloma is initially rich in immune cells and is highly vascularized (it is referred to as a cellular granuloma), which facilitates drug distribution into the core of the lesion. Bacilli reside extracellularly and in activated and foamy macrophages. As the granuloma matures, it begins to necrotize from the centre outwards, and vascularization is gradually destroyed, although the fibrotic rim and cellular layer remain densely vascularized. Bacilli can be found extracellularly in the necrotic caseum and in immune cells. When an expanding granuloma meets an airway, the necrotic centre fuses with the airway structure to form a cavity. Mycobacteria are found extracellularly in the cavity caseum and intracellularly in macrophages, foamy macrophages and neutrophils. Both intracellular and extracellular bacteria are released at the luminal side of the cavity and later appear in sputum. Image is modified, with permission, from REF. © (2013) Elsevier.
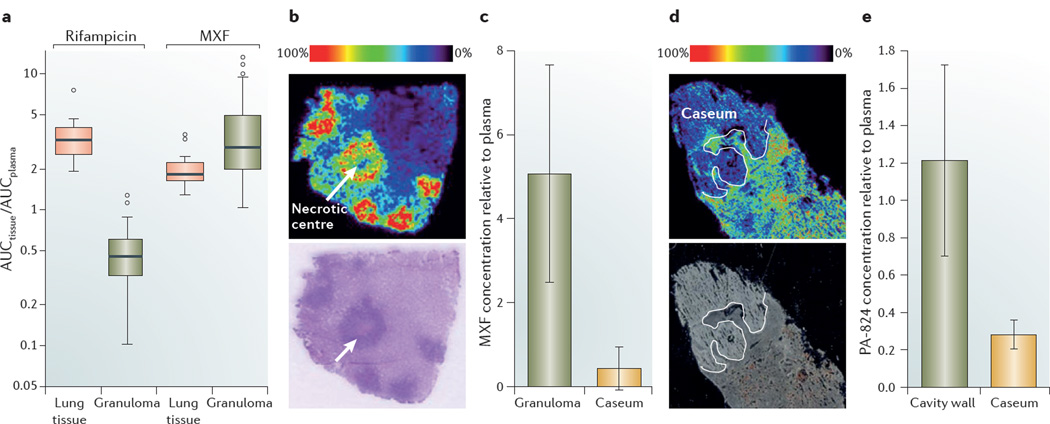
a | Boxplots of rifampicin and moxifloxacin (MXF) concentrations in lung tissue and cellular granulomas, relative to plasma concentrations, which show that both drugs are efficiently distributed in healthy lung tissue. Rifampicin concentrations are significantly lower in granulomas than in healthy lung tissue, whereas the opposite is observed for MXF. The box width is the interquartile range and the horizontal line marks the median value. The T-bars indicate the maximum and minimum of ratios within 1.5x the upper and lower quartiles, respectively. Observed datapoints that fall outside this range are represented by open circles. b | A mass spectrometry image that shows the distribution of MXF in necrotizing rabbit granulomas. The panel contains an ion map (upper panel) and the corresponding hematoxylin and eosin-stained section (lower panel). A signal intensity of 0% corresponds to minimum signal, whereas 100% is assigned to the maximum signal, which, in the case of MXF, corresponds to the cellular cuff of granulomas. The signal responds linearly up to 1 nmol, which is several orders of magnitude higher than the therapeutically relevant drug concentrations that are achieved in tissues. The ion map clearly shows lower drug levels in caseum compared to the surrounding cellular region, which highlights the poor diffusion capacity of MXF in the necrotic core, where extracellular bacilli reside. c | Absolute concentrations of MXF were measured by HPLC coupled to tandem mass spectronomy (LC–MS/MS) in tissue homogenates of caseum and the cellular fraction of granulomas, and these are shown relative to the absolute drug concentration measured in plasma at the time of rabbit necropsy. The bar graph shows the MXF concentration in granuloma and caseum relative to plasma at 2 hours post-dose, which confirms that the drug distributes more efficiently in the cellular fraction of the granuloma than in caseum (V.D., unpublished observations). d | Distribution of the nitroimidazole PA 824 in a large rabbit necrotic granuloma. Similarly to MXF, the ion map (upper panel) shows that PA 824 has limited penetration in caseum. The lower panel is an optical image of the same tissue section prior to matrix coating and imaging. e | Absolute concentrations of PA 824 were measured by LC–MS/MS in the caseum and cellular wall of three cavities that were found in the same animal at the time of necropsy, and these are shown relative to the absolute drug concentration measured in plasma. The concentration of PA 824 in the cavity wall is higher than in caseum (V.D., unpublished observations), which confirms the results of MALDI–MS (part d). Graph in part a is reproduced, with permission, from REF. © (2012) American Society for Microbiology. The images in part b are reproduced, with permission, from REF. © (2011) American Cell Society. Images in part d are reproduced, with permission, from REF. © (2012) Science Direct.
References
-
- World Health Organization. Global Tuberculosis Report. WHO; 2012.
-
- Bass JB, Jr, et al. Treatment of tuberculosis and tuberculosis infection in adults and children. American Thoracic Society and the Centers for Disease Control and Prevention. Am. J. Respir. Crit. Care Med. 1994;149:1359–1374. - PubMed
-
- Bates JH, Nardell E. Institutional control measures for tuberculosis in the era of multiple drug resistance: ACCP/ATS Consensus Conference. Chest. 1995;108:1690–1710. - PubMed
-
- Monedero I, Caminero JA. MDR-/XDR TB management: what it was, current standards and what is ahead. Expert Rev. Respir. Med. 2009;3:133–145. - PubMed
-
- Caminero JA, Sotgiu G, Zumla A, Migliori GB. Best drug treatment for multidrug-resistant and extensively drug-resistant tuberculosis. Lancet Infect. Dis. 2010;10:621–629. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
