

Effects of preoperative hypoxia on white matter injury associated with cardiopulmonary bypass in a rodent hypoxic and brain slice model
- PMID: 24488087
- PMCID: PMC3992169
- DOI: 10.1038/pr.2014.9
Effects of preoperative hypoxia on white matter injury associated with cardiopulmonary bypass in a rodent hypoxic and brain slice model
Abstract
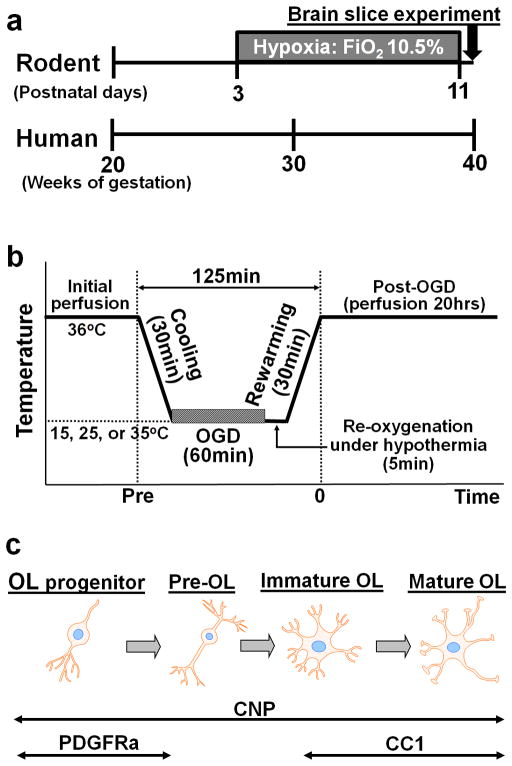
Background: White matter (WM) injury is common after cardiopulmonary bypass or deep hypothermic circulatory arrest in neonates who have cerebral immaturity secondary to in utero hypoxia. The mechanism remains unknown. We investigated effects of preoperative hypoxia on deep hypothermic circulatory arrest-induced WM injury using a combined experimental paradigm in rodents.
Methods: Mice were exposed to hypoxia (prehypoxia). Oxygen-glucose deprivation was performed under three temperatures to simulate brain conditions of deep hypothermic circulatory arrest including ischemia-reperfusion/reoxygenation under hypothermia.
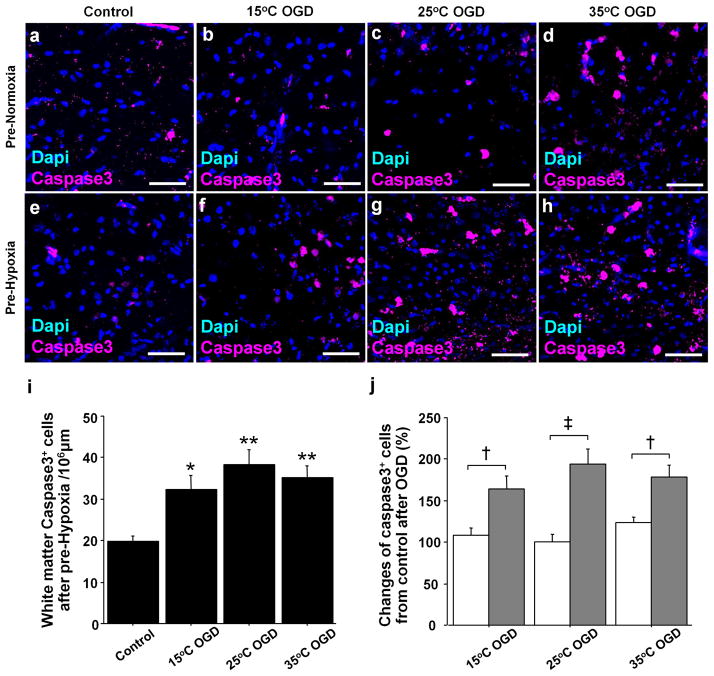
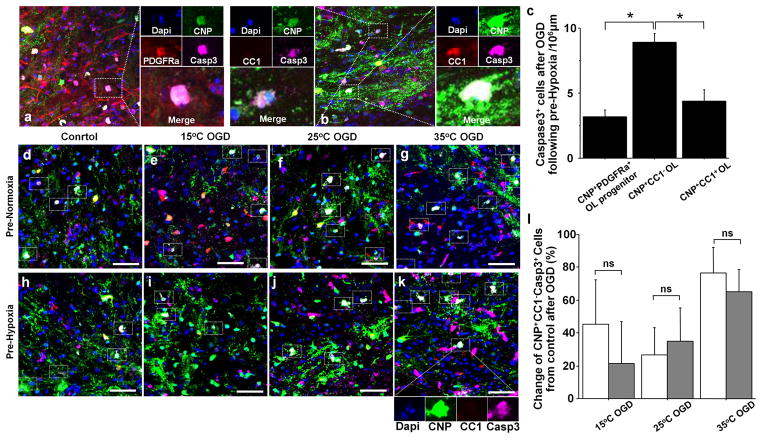
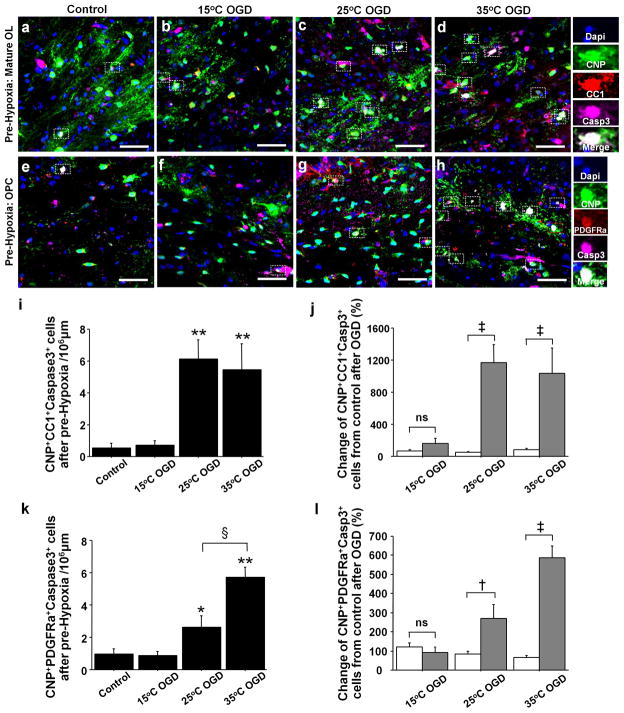
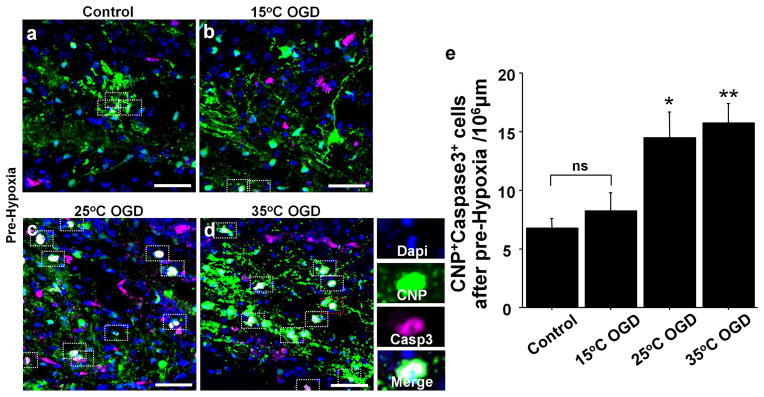
Results: WM injury in prenormoxia was identified after 35 °C-oxygen-glucose deprivation. In prehypoxia, injury was displayed in all groups. Among oligodendrocyte stages, the preoligodendrocyte was the most susceptible, while the oligodendrocyte progenitor was resistant to insult. When effects of prehypoxia were assessed, injury of mature oligodendrocytes and oligodendrocyte progenitors in prehypoxia significantly increased as compared with prenormoxia, indicating that mature oligodendrocytes and progenitors that had developed under hypoxia had greater vulnerability. Conversely, damage of oligodendrocyte progenitors in prehypoxia were not identified after 15 °C-oxygen-glucose deprivation, suggesting that susceptible oligodendrocytes exposed to hypoxia are protected by deep hypothermia.
Conclusion: Developmental alterations due to hypoxia result in an increased WM susceptibility to injury. Promoting WM regeneration by oligodendrocyte progenitors after earlier surgery using deep hypothermia is the most promising approach for successful WM development in congenital heart disease patients.
Figures
Similar articles
-
Hypoxia diminishes the protective function of white-matter astrocytes in the developing brain.J Thorac Cardiovasc Surg. 2016 Jan;151(1):265-72.e1-3. doi: 10.1016/j.jtcvs.2015.08.076. Epub 2015 Sep 26. J Thorac Cardiovasc Surg. 2016. PMID: 26412317 Free PMC article.
-
Rodent brain slice model for the study of white matter injury.J Thorac Cardiovasc Surg. 2013 Dec;146(6):1526-1533.e1. doi: 10.1016/j.jtcvs.2013.02.071. Epub 2013 Mar 27. J Thorac Cardiovasc Surg. 2013. PMID: 23540655 Free PMC article.
-
Inhibition of microglial activation by minocycline reduced preoligodendrocyte injury in a neonatal rat brain slice model.J Thorac Cardiovasc Surg. 2018 Dec;156(6):2271-2280. doi: 10.1016/j.jtcvs.2018.06.038. Epub 2018 Jul 18. J Thorac Cardiovasc Surg. 2018. PMID: 30121135
-
Cerebral injury during paediatric heart surgery: perfusion issues.Perfusion. 2004 Jul;19(4):221-8. doi: 10.1191/0267659104pf742oa. Perfusion. 2004. PMID: 15376766 Review.
-
The postoperative care of adult patients exposed to deep hypothermic circulatory arrest.Semin Cardiothorac Vasc Anesth. 2007 Mar;11(1):77-85. doi: 10.1177/1089253206298010. Semin Cardiothorac Vasc Anesth. 2007. PMID: 17484176 Review.
Cited by
-
White Matter Brain Development after Exposure to Circulating Cell-Free Hemoglobin and Hyperoxia in a Rat Pup Model.Dev Neurosci. 2019;41(3-4):234-246. doi: 10.1159/000505206. Epub 2020 Jan 28. Dev Neurosci. 2019. PMID: 31991415 Free PMC article.
-
Congenital cardiac anomalies and white matter injury.Trends Neurosci. 2015 Jun;38(6):353-63. doi: 10.1016/j.tins.2015.04.001. Epub 2015 May 1. Trends Neurosci. 2015. PMID: 25939892 Free PMC article. Review.
-
Symptomatic newborn coronary fistula repair without cardiopulmonary bypass.JTCVS Tech. 2022 Nov 17;17:153-154. doi: 10.1016/j.xjtc.2022.11.003. eCollection 2023 Feb. JTCVS Tech. 2022. PMID: 36820342 Free PMC article. No abstract available.
-
Microstructural Alterations and Oligodendrocyte Dysmaturation in White Matter After Cardiopulmonary Bypass in a Juvenile Porcine Model.J Am Heart Assoc. 2017 Aug 15;6(8):e005997. doi: 10.1161/JAHA.117.005997. J Am Heart Assoc. 2017. PMID: 28862938 Free PMC article.
-
Individual Assessment of Perioperative Brain Growth Trajectories in Infants With Congenital Heart Disease: Correlation With Clinical and Surgical Risk Factors.J Am Heart Assoc. 2023 Jul 18;12(14):e028565. doi: 10.1161/JAHA.122.028565. Epub 2023 Jul 8. J Am Heart Assoc. 2023. PMID: 37421268 Free PMC article.
References
-
- Kaltman JR, Andropoulos DB, Checchia PA, et al. Report of the pediatric heart network and national heart, lung, and blood institute working group on the perioperative management of congenital heart disease. Circulation. 2010;121:2766–72. - PubMed
-
- Wernovsky G. Current insights regarding neurological and developmental abnormalities in children and young adults with complex congenital cardiac disease. Cardiol Young. 2006;16 (Suppl 1):92–104. - PubMed
-
- Gaynor JW. Periventricular leukomalacia following neonatal and infant cardiac surgery. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:133–40. - PubMed
-
- Miller SP, McQuillen PS, Hamrick S, et al. Abnormal brain development in newborns with congenital heart disease. N Engl J Med. 2007;357:1928–38. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
