

Use of the quality management system "JACIE" and outcome after hematopoietic stem cell transplantation
- PMID: 24488562
- PMCID: PMC4008105
- DOI: 10.3324/haematol.2013.096461
Use of the quality management system "JACIE" and outcome after hematopoietic stem cell transplantation
Abstract
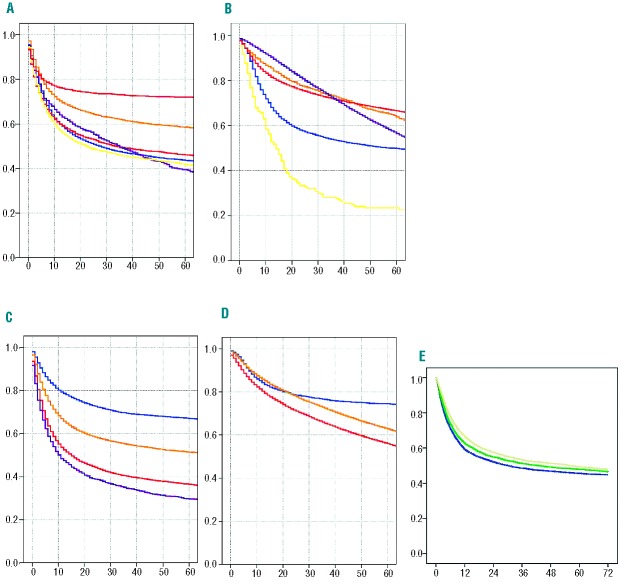
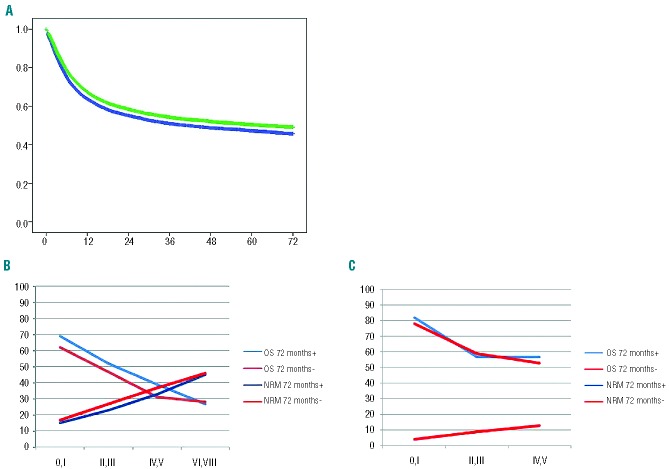
Competent authorities, healthcare payers and hospitals devote increasing resources to quality management systems but scientific analyses searching for an impact of these systems on clinical outcome remain scarce. Earlier data indicated a stepwise improvement in outcome after allogeneic hematopoietic stem cell transplantation with each phase of the accreditation process for the quality management system "JACIE". We therefore tested the hypothesis that working towards and achieving "JACIE" accreditation would accelerate improvement in outcome over calendar time. Overall mortality of the entire cohort of 107,904 patients who had a transplant (41,623 allogeneic, 39%; 66,281 autologous, 61%) between 1999 and 2006 decreased over the 14-year observation period by a factor of 0.63 per 10 years (hazard ratio: 0.63; 0.58-0.69). Considering "JACIE"-accredited centers as those with programs having achieved accreditation by November 2012, at the latest, this improvement was significantly faster in "JACIE"-accredited centers than in non-accredited centers (approximately 5.3% per year for 49,459 patients versus approximately 3.5% per year for 58,445 patients, respectively; hazard ratio: 0.83; 0.71-0.97). As a result, relapse-free survival (hazard ratio 0.85; 0.75-0.95) and overall survival (hazard ratio 0.86; 0.76-0.98) were significantly higher at 72 months for those patients transplanted in the 162 "JACIE"-accredited centers. No significant effects were observed after autologous transplants (hazard ratio 1.06; 0.99-1.13). Hence, working towards implementation of a quality management system triggers a dynamic process associated with a steeper reduction in mortality over the years and a significantly improved survival after allogeneic stem cell transplantation. Our data support the use of a quality management system for complex medical procedures.
Figures
References
-
- Buzzell RD, Gale BD, The PIMS Principles. Linking Strategy to Performance. New York: The Free Press; 1987
-
- Ryan J. Making the economic case for quality. An ASQ white paper. American Society for Quality; (cited 2013 March 14). Available from: http://rube.asq.org/pdf/economic-case/economic-case.pdf
-
- Hendricks KB, Singhal VR. Does implementing an effective TQM program actually improve operating performance¿ Empirical evidence from firms that have won quality awards. Manage Sci. 1997;43(9):1258–74
-
- Cole RE. What really happened to Toyota¿ MIT Sloan Manage Rev. 2011;52(2):28–35
-
- Punnakitikashem P, Laosirihongthong T, Adebanjo D, McLean MW. A study of quality management practices in TQM and non-TQM firms: findings from the ASEAN automotive industry. Int J Qual Reliab Manag. 2010;27(9):1021–35
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
