

Clinical use of ultrasensitive cardiac troponin I assay in intermediate- and high-risk surgery patients
- PMID: 24489430
- PMCID: PMC3893737
- DOI: 10.1155/2013/169356
Clinical use of ultrasensitive cardiac troponin I assay in intermediate- and high-risk surgery patients
Abstract
Background: Cardiac troponin levels have been reported to add value in the detection of cardiovascular complications in noncardiac surgery. A sensitive cardiac troponin I (cTnI) assay could provide more accurate prognostic information.
Methods: This study prospectively enrolled 142 patients with at least one Revised Cardiac Risk Index risk factor who underwent noncardiac surgery. cTnI levels were measured postoperatively. Short-term cardiac outcome predictors were evaluated.
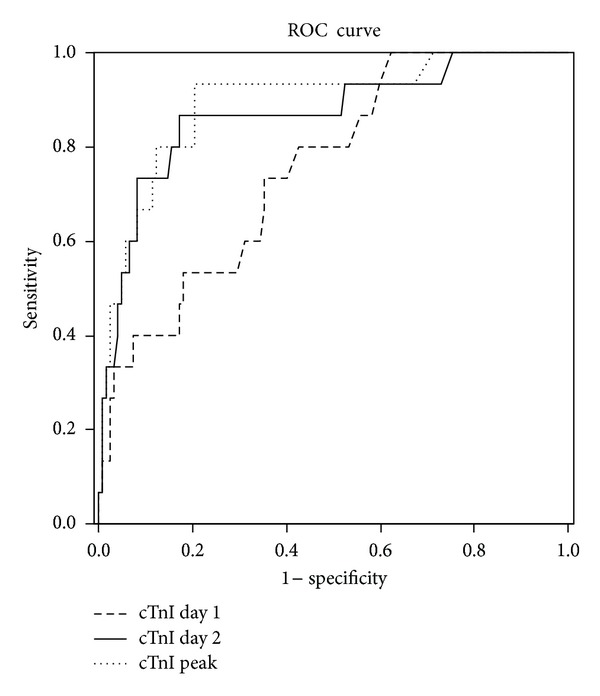
Results: cTnI elevation was observed in 47 patients, among whom 14 were diagnosed as having myocardial infarction (MI). After 30 days, 16 patients had major adverse cardiac events (MACE). Excluding patients with a final diagnosis of MI, predictors of cTnI elevation included dialysis, history of heart failure, transoperative major bleeding, and elevated levels of pre- and postoperative N-terminal pro-B-type natriuretic peptide (NT-proBNP). Maximal cTnI values showed the highest sensitivity (94%), specificity (75%), and overall accuracy (AUC 0.89; 95% CI 0.80-0.98) for postoperative MACE. Postoperative cTnI peak level (OR 9.4; 95% CI 2.3-39.2) and a preoperative NT-proBNP level ≥917 pg/mL (OR 3.47; 95% CI 1.05-11.6) were independent risk factors for MACE.
Conclusions: cTnI was shown to be an independent prognostic factor for cardiac outcomes and should be considered as a component of perioperative risk assessment.
Figures


References
-
- Mangano DT, Browner WS, Hollenberg M, London MJ, Tubau JF, Tateo IM. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. The New England Journal of Medicine. 1990;323(26):1781–1788. - PubMed
-
- Ashton CM, Petersen NJ, Wray NP, et al. The incidence of perioperative myocardial infarction in men undergoing noncardiac surgery. Annals of Internal Medicine. 1993;118(7):504–510. - PubMed
-
- Badner NH, Knill RL, Brown JE, Novick TV, Gelb AW. Myocardial infarction after noncardiac surgery. Anesthesiology. 1998;88(3):572–578. - PubMed
-
- Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043–1049. - PubMed
-
- Devereaux PJ, Yang H, Yusuf S, et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. The Lancet. 2008;371:1839–1847. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
