

Recommendations for the empirical treatment of complicated urinary tract infections using surveillance data on antimicrobial resistance in the Netherlands
- PMID: 24489755
- PMCID: PMC3904917
- DOI: 10.1371/journal.pone.0086634
Recommendations for the empirical treatment of complicated urinary tract infections using surveillance data on antimicrobial resistance in the Netherlands
Erratum in
- PLoS One. 2014;9(9):e107785. van Hall, Maurine A Leverstein- [corrected to Leverstein-van Hall, Maurine A]
Abstract
Background: Complicated urinary tract infections (c-UTIs) are among the most common nosocomial infections and a substantial part of the antimicrobial agents used in hospitals is for the treatment of c-UTIs. Data from surveillance can be used to guide the empirical treatment choices of clinicians when treating c-UTIs. We therefore used nation-wide surveillance data to evaluate antimicrobial coverage of agents for the treatment of c-UTI in the Netherlands.
Methods: We included the first isolate per patient of urine samples of hospitalised patients collected by the Infectious Disease Surveillance Information System for Antibiotic Resistance (ISIS-AR) in 2012, and determined the probability of inadequate coverage for antimicrobial agents based on species distribution and susceptibility. Analyses were repeated for various patient groups and hospital settings.
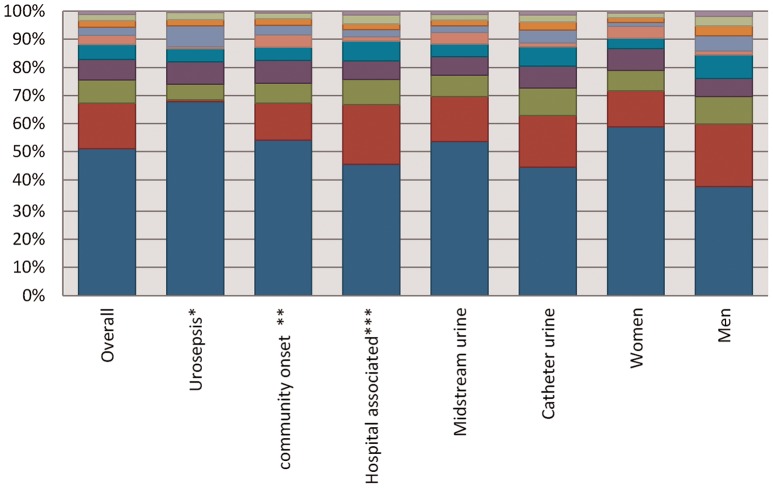
Results: The most prevalent bacteria in 27,922 isolates of 23,357 patients were Escherichia coli (47%), Enterococcus spp. (14%), Proteus mirabilis (8%), and Klebsiella pneumoniae (7%). For all species combined, the probability of inadequate coverage was <5% for amoxicillin or amoxicillin-clavulanic acid combined with gentamicin and the carbapenems. When including gram-negative bacteria only, the probability of inadequate coverage was 4.0%, 2.7%, 2.3% and 1.7%, respectively, for amoxicillin, amoxicillin-clavulanic acid, a second or a third generation cephalosporin in combination with gentamicin, and the carbapenems (0.4%). There were only small variations in results among different patient groups and hospital settings.
Conclusions: When excluding Enterococcus spp., considered as less virulent, and the carbapenems, considered as last-resort drugs, empirical treatment for c-UTI with the best chance of adequate coverage are one of the studied beta-lactam-gentamicin combinations. This study demonstrates the applicability of routine surveillance data for up-to-date clinical practice guidelines on empirical antimicrobial therapy, essential in patient care given the evolving bacterial susceptibility.
Conflict of interest statement
Figures
References
-
- van der Kooi TI, Mannien J, Wille JC, van Benthem BH (2010) Prevalence of nosocomial infections in The Netherlands, 2007–2008: results of the first four national studies. J Hosp Infect 75: 168–172. - PubMed
-
- Wagenlehner FM, Naber KG (2006) Treatment of bacterial urinary tract infections: presence and future. Eur Urol 49: 235–244. - PubMed
-
- Geerlings SE, van den Broek PJ, van Haarst EP, Vleming LJ, van Haaren KM, et al. (2006) Optimisation of the antibiotic policy in the Netherlands. The SWAB guideline for antimicrobial treatment of complicated urinary tract infections [In Dutch]. Ned Tijdschr Geneeskd 150: 2370–2376. - PubMed
-
- Johnson JR, Kuskowski MA, Gajewski A, Sahm DF, Karlowsky JA (2004) Virulence characteristics and phylogenetic background of multidrug-resistant and antimicrobial-susceptible clinical isolates of Escherichia coli from across the United States, 2000–2001. J Infect Dis 190: 1739–1744. - PubMed
-
- Paterson DL, Mulazimoglu L, Casellas JM, Ko WC, Goossens H, et al. (2000) Epidemiology of ciprofloxacin resistance and its relationship to extended-spectrum beta-lactamase production in Klebsiella pneumoniae isolates causing bacteremia. Clin Infect Dis 30: 473–478. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
