

The cost and cost-effectiveness of scaling up screening and treatment of syphilis in pregnancy: a model
- PMID: 24489931
- PMCID: PMC3906198
- DOI: 10.1371/journal.pone.0087510
The cost and cost-effectiveness of scaling up screening and treatment of syphilis in pregnancy: a model
Abstract
Background: Syphilis in pregnancy imposes a significant global health and economic burden. More than half of cases result in serious adverse events, including infant mortality and infection. The annual global burden from mother-to-child transmission (MTCT) of syphilis is estimated at 3.6 million disability-adjusted life years (DALYs) and $309 million in medical costs. Syphilis screening and treatment is simple, effective, and affordable, yet, worldwide, most pregnant women do not receive these services. We assessed cost-effectiveness of scaling-up syphilis screening and treatment in existing antenatal care (ANC) programs in various programmatic, epidemiologic, and economic contexts.
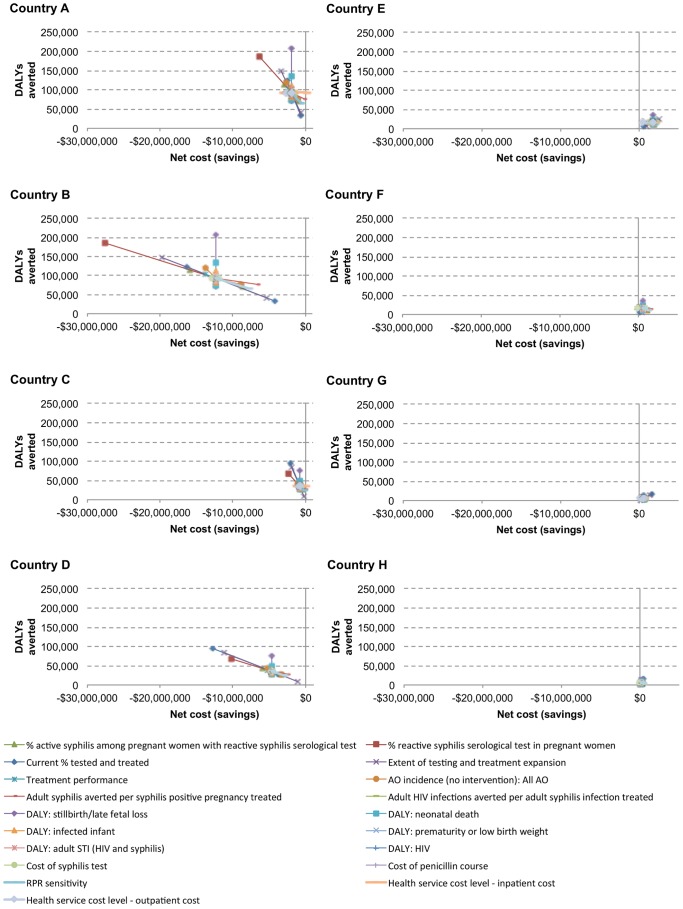
Methods and findings: We modeled the cost, health impact, and cost-effectiveness of expanded syphilis screening and treatment in ANC, compared to current services, for 1,000,000 pregnancies per year over four years. We defined eight generic country scenarios by systematically varying three factors: current maternal syphilis testing and treatment coverage, syphilis prevalence in pregnant women, and the cost of healthcare. We calculated program and net costs, DALYs averted, and net costs per DALY averted over four years in each scenario. Program costs are estimated at $4,142,287 - $8,235,796 per million pregnant women (2010 USD). Net costs, adjusted for averted medical care and current services, range from net savings of $12,261,250 to net costs of $1,736,807. The program averts an estimated 5,754 - 93,484 DALYs, yielding net savings in four scenarios, and a cost per DALY averted of $24 - $111 in the four scenarios with net costs. Results were robust in sensitivity analyses.
Conclusions: Eliminating MTCT of syphilis through expanded screening and treatment in ANC is likely to be highly cost-effective by WHO-defined thresholds in a wide range of settings. Countries with high prevalence, low current service coverage, and high healthcare cost would benefit most. Future analyses can be tailored to countries using local epidemiologic and programmatic data.
Conflict of interest statement
Figures
References
-
- World Health Organization (2012) Investment case for eliminating mother-to-child transmission of syphilis: Promoting better maternal and child health and stronger health systems. Geneva, Switzerland.
-
- Hawkes S, Matin N, Broutet N, Low N (2011) Effectiveness of interventions to improve screening for syphilis in pregnancy: a systematic review and meta-analysis. Lancet Infect Dis 11: 684–691. - PubMed
-
- Blandford JM, Gift TL, Vasaikar S, Mwesigwa-Kayongo D, Dlali P, et al. (2007) Cost-effectiveness of on-site antenatal screening to prevent congenital syphilis in rural eastern Cape Province, Republic of South Africa. Sexually transmitted diseases 34: S61–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
