

Imaging of cardiac valves by computed tomography
- PMID: 24490107
- PMCID: PMC3893874
- DOI: 10.1155/2013/270579
Imaging of cardiac valves by computed tomography
Abstract
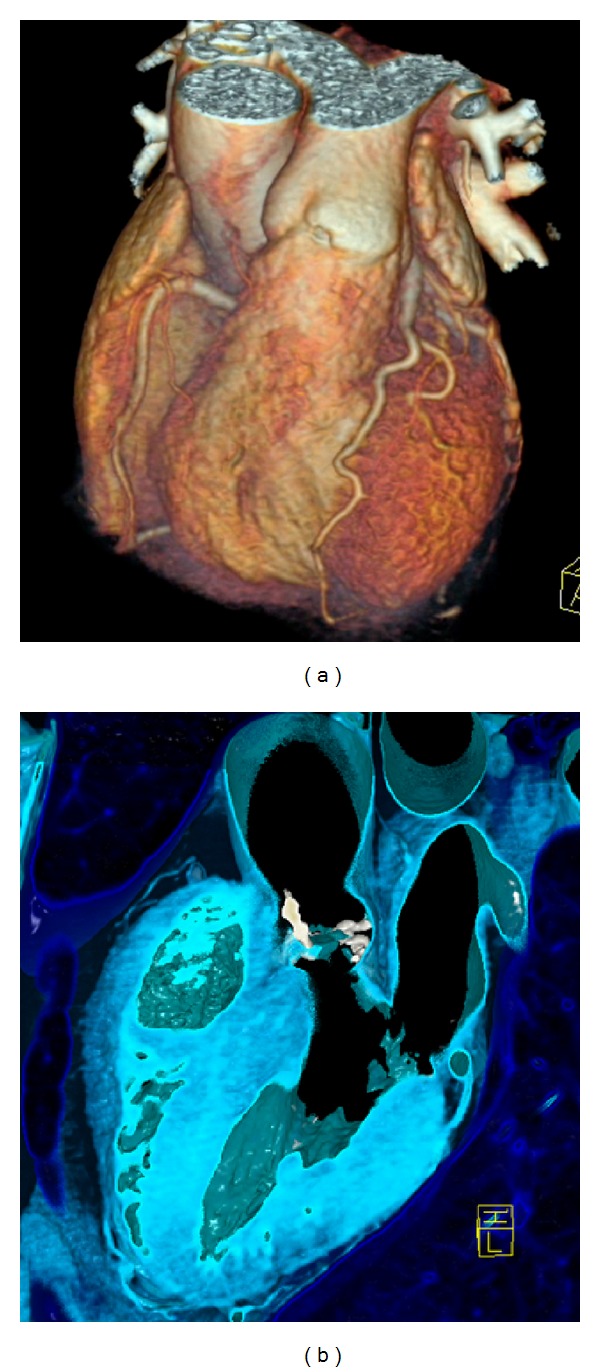
This paper describes "how to" examine cardiac valves with computed tomography, the normal, diseased valves, and prosthetic valves. A review of current scientific literature is provided. Firstly, technical basics, "how to" perform and optimize a multislice CT scan and "how to" interpret valves on CT images are outlined. Then, diagnostic imaging of the entire spectrum of specific valvular disease by CT, including prosthetic heart valves, is highlighted. The last part gives a guide "how to" use CT for planning of transcatheter aortic valve implantation (TAVI), an emerging effective treatment option for patients with severe aortic stenosis. A special focus is placed on clinical applications of cardiac CT in the context of valvular disease.
Figures



References
-
- Feuchtner G, Goetti R, Plass A, et al. Dual-step prospective ECG-triggered 128-slice dual-source ct for evaluation of coronary arteries and cardiac function without heart rate control: a technical note. European Radiology. 2010;20(9):2092–2099. - PubMed
-
- Achenbach S, Marwan M, Ropers D, et al. Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. European Heart Journal. 2010;31(3):340–346. - PubMed
-
- Leschka S, Stolzmann P, Desbiolles L, et al. Diagnostic accuracy of high-pitch dual-source CT for the assessment of coronary stenoses: first experience. European Radiology. 2009;19(12):2896–2903. - PubMed
-
- Alkadhi H, Stolzmann P, Desbiolles L, et al. Low-dose, 128-slice, dual-source CT coronary angiography: accuracy and radiation dose of the high-pitch and the step-and-shoot mode. Heart. 2010;96(12):933–938. - PubMed
-
- Marwan M, Pflederer T, Schepis T, et al. Accuracy of dual-source computed tomography to identify significant coronary artery disease in patients with atrial fibrillation: comparison with coronary angiography. European Heart Journal. 2010;31(18):2230–2237. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
