

Intraperitoneal chemotherapy for peritoneal surface malignancy: experience with 1,000 patients
- PMID: 24491244
- PMCID: PMC3965636
- DOI: 10.1016/j.jamcollsurg.2013.12.013
Intraperitoneal chemotherapy for peritoneal surface malignancy: experience with 1,000 patients
Abstract
Background: Peritoneal dissemination of abdominal malignancy (carcinomatosis) has a clinical course marked by bowel obstruction and death; it traditionally does not respond well to systemic therapy and has been approached with nihilism. To treat carcinomatosis, we use cytoreductive surgery (CS) with hyperthermic intraperitoneal chemotherapy (HIPEC).
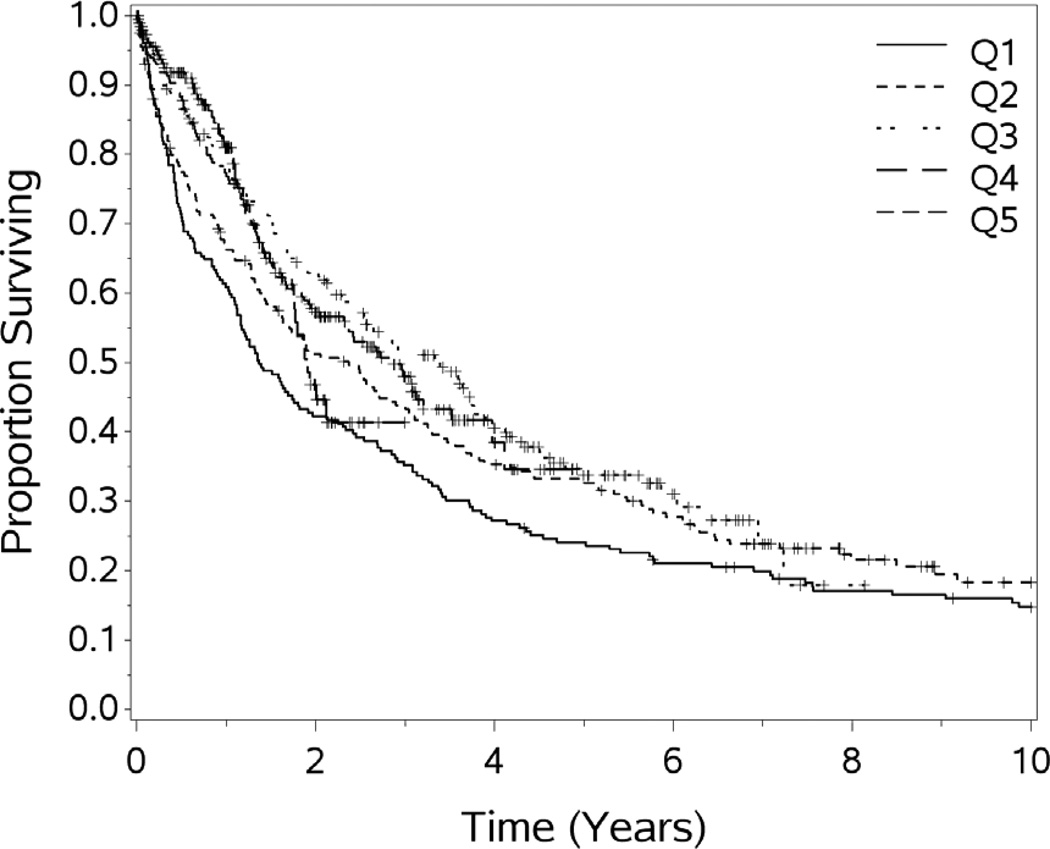
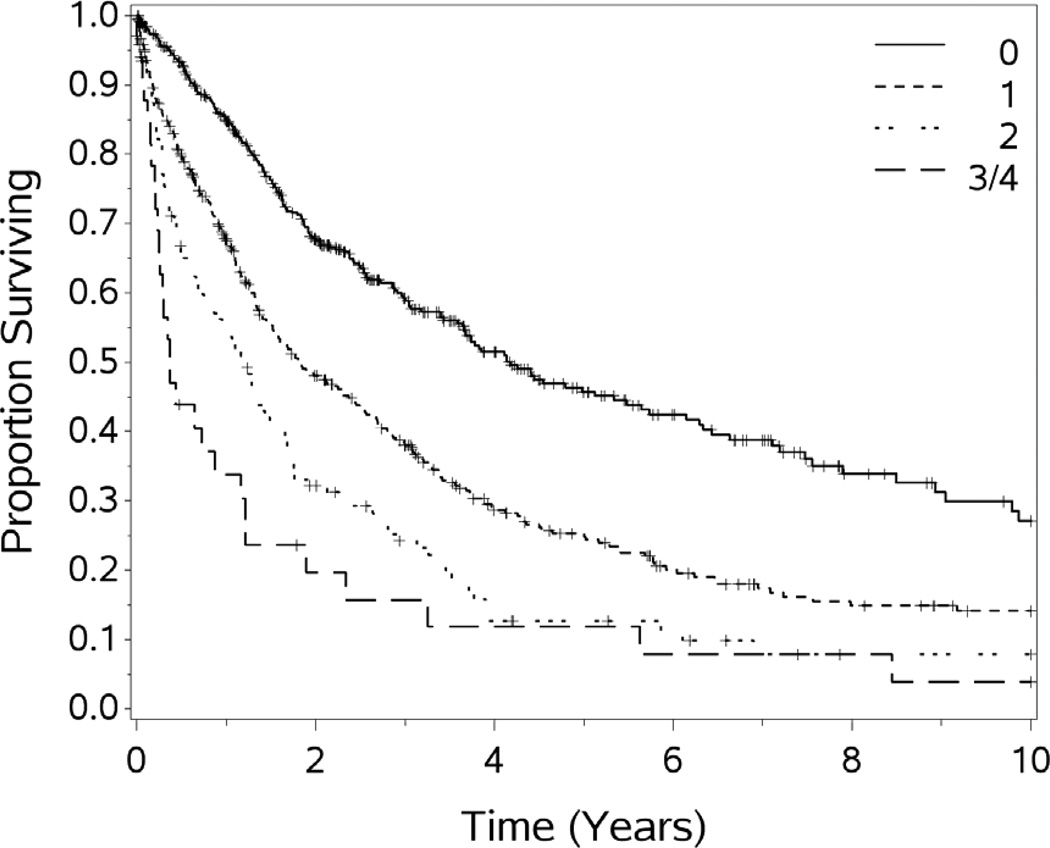
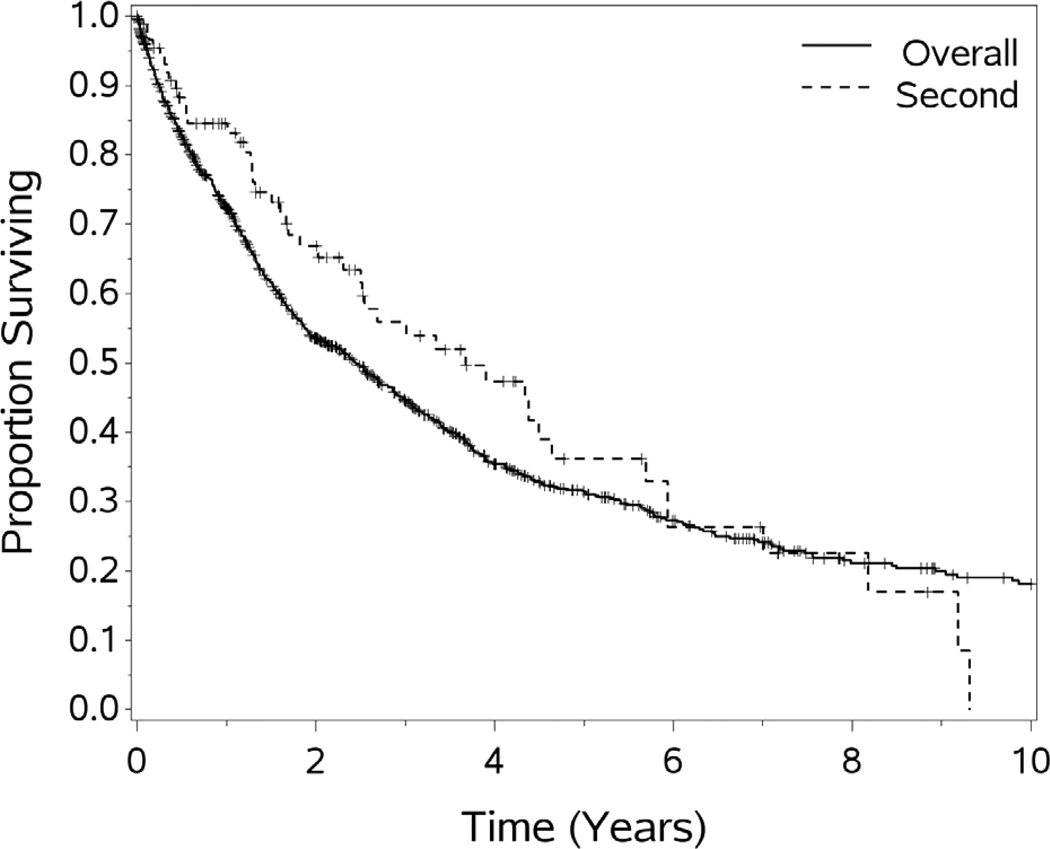
Methods: A prospective database of patients has been maintained since 1992. Patients with biopsy-proven peritoneal surface disease were uniformly evaluated for, and treated with, CS and HIPEC. Patient demographics, performance status (Eastern Cooperative Oncology Group), resection status, and peritoneal surface disease were classified according to primary site. Univariate and multivariate analyses were performed. The experience was divided into quintiles and outcomes compared.
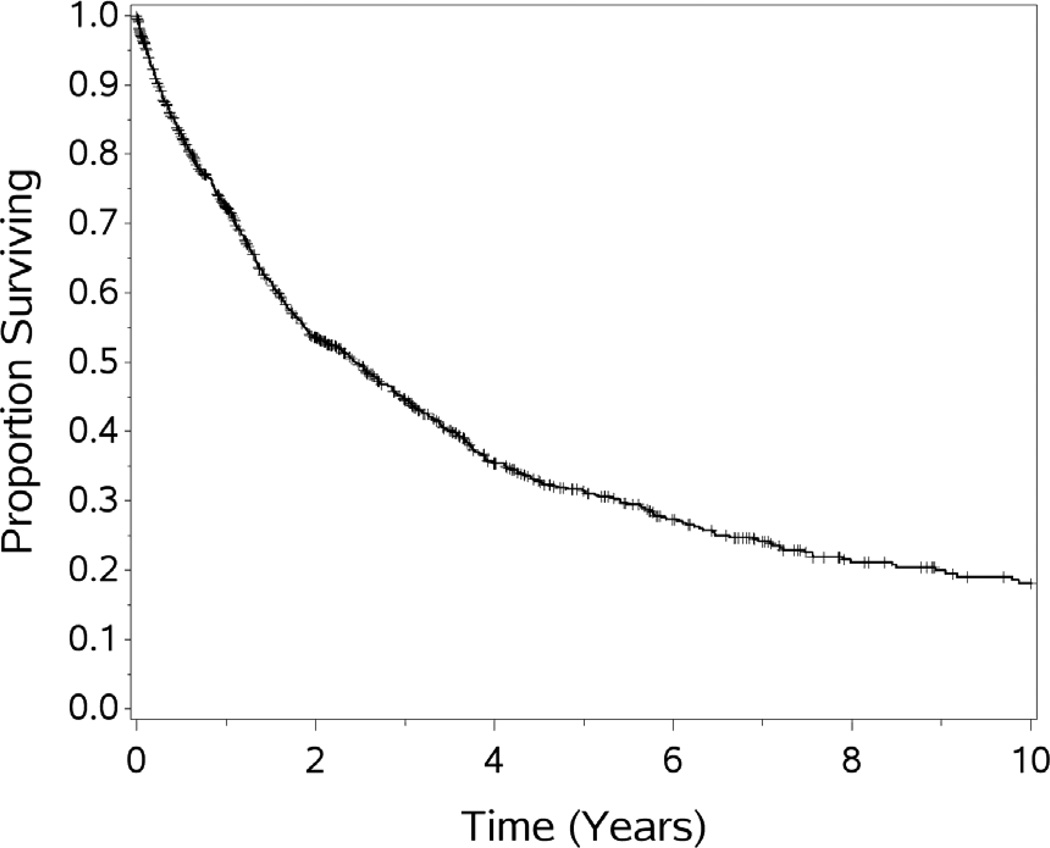
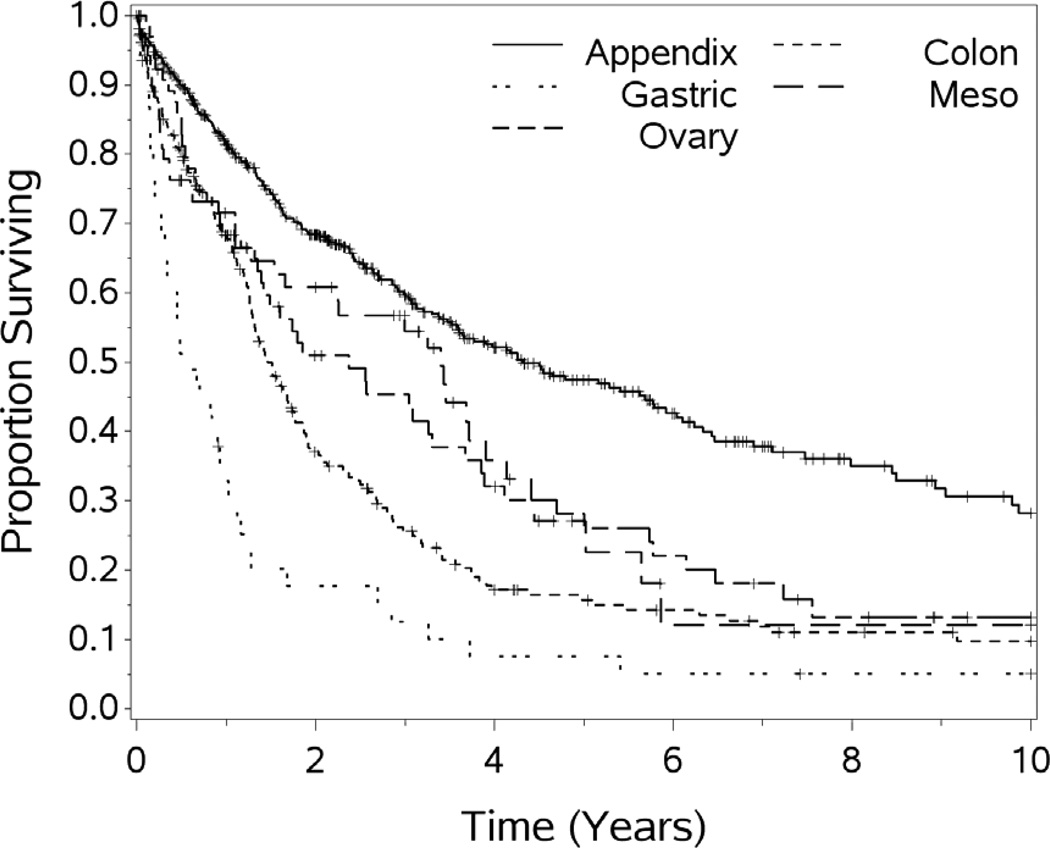
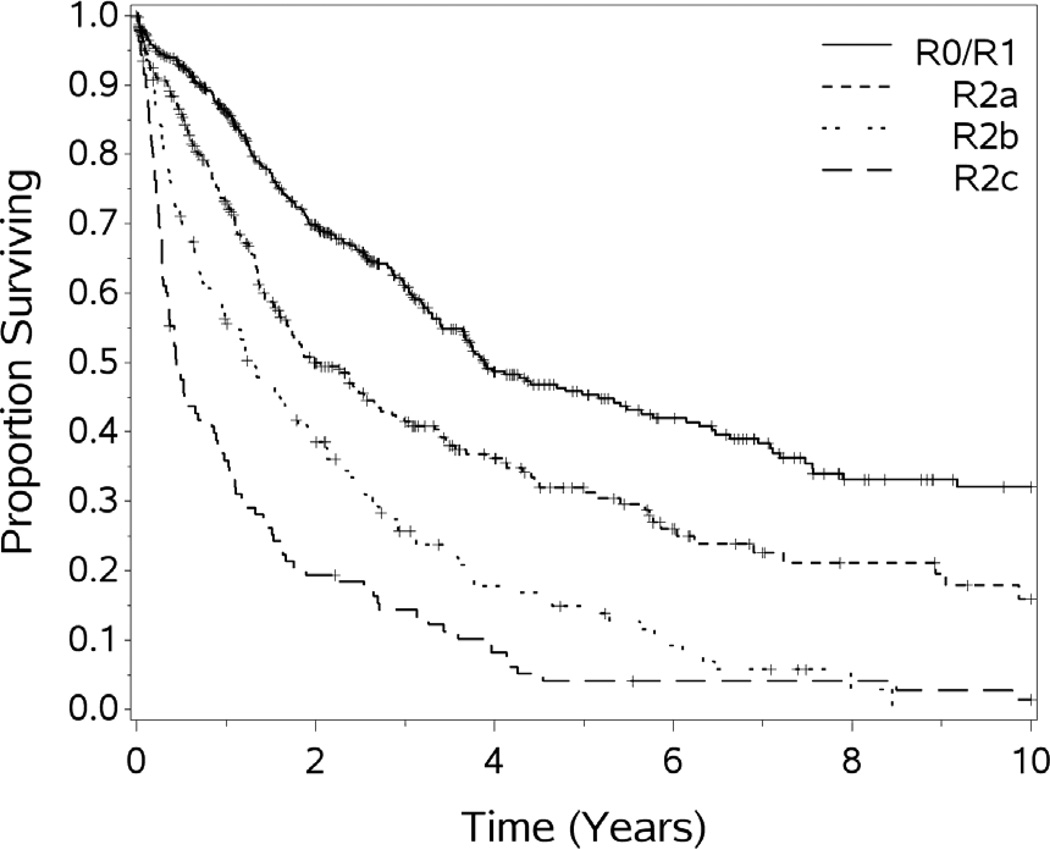
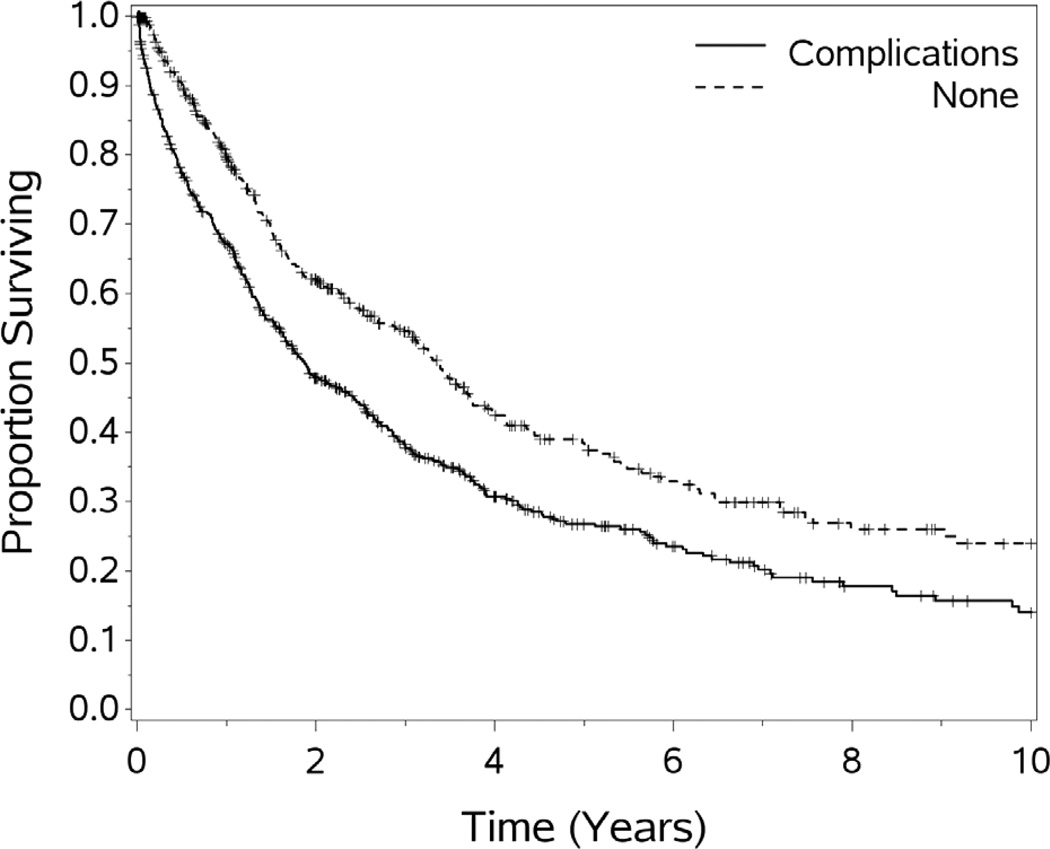
Results: Between 1991 and 2013, a total of 1,000 patients underwent 1,097 HIPEC procedures. Mean age was 52.9 years and 53.1% were female. Primary tumor site was appendix in 472 (47.2%), colorectal in 248 (24.8%), mesothelioma in 72 (7.2%), ovary in 69 (6.9%), gastric in 46 (4.6%), and other in 97 (9.7%). Thirty-day mortality rate was 3.8% and median hospital stay was 8 days. Median overall survival was 29.4 months, with a 5-year survival rate of 32.5%. Factors correlating with improved survival on univariate and multivariate analysis (p ≤ 0.0001 for each) were preoperative performance status, primary tumor type, resection status, and experience quintile (p = 0.04). For the 5 quintiles, the 1- and 5-year survival rates, as well as the complete cytoreduction score (R0, R1, R2a) have increased, and transfusions, stoma creations, and complications have all decreased significantly (p < .001 for all).
Conclusions: This largest reported single-center experience with CS and HIPEC demonstrates that prognostic factors include primary site, performance status, completeness of resection, and institutional experience. The data show that outcomes have improved over time, with more complete cytoreduction and fewer serious complications, transfusions, and stomas. This was due to better patient selection and increased operative experience. Cytoreductive surgery with HIPEC represents a substantial improvement in outcomes compared with historical series, and shows that meaningful long-term survival is possible for selected carcinomatosis patients. Multi-institutional cooperative trials are needed to refine the use of CS and HIPEC.
Copyright © 2014 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2014 Apr;218(4):586-7. doi: 10.1016/j.jamcollsurg.2014.01.010. J Am Coll Surg. 2014. PMID: 24655844 No abstract available.
References
-
- Sadeghi B, Arvieux C, Glehen O, et al. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer. 2000;88:358–363. - PubMed
-
- Torisu M, Katano M, Kimura Y, et al. New approach to management of malignant ascitis with a streptococcal preparation OK 432: improvement of host immunity and prolongation of survival. Surgery. 1983;93:357–353. - PubMed
-
- Hendren SK, Hahn SM, Spitz FR, et al. Phase II trial of debulking surgery and photodynamic therapy for disseminated intraperitoneal tumors. Annals of Surgical Oncoogyl. 2001;8:65–71. - PubMed
-
- Sindelar WF, DeLaney TF, Tochner Z, et al. Technique of photodynamic therapy for disseminated intraperitoneal malignant neoplasms. Phase I study. Archives of Surgery. 1991;126:318–324. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
