

The influence of prior abiraterone treatment on the clinical activity of docetaxel in men with metastatic castration-resistant prostate cancer
- PMID: 24491307
- PMCID: PMC4110192
- DOI: 10.1016/j.eururo.2014.01.018
The influence of prior abiraterone treatment on the clinical activity of docetaxel in men with metastatic castration-resistant prostate cancer
Abstract
Background: Taxanes may partly mediate their effect in castration-resistant prostate cancer (CRPC) through disruption of androgen-receptor trafficking along microtubules. This raises the possibility of cross-resistance between androgen-directed agents and docetaxel.
Objective: To evaluate docetaxel efficacy after abiraterone treatment in CRPC patients.
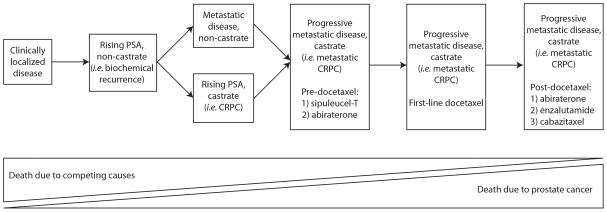
Design, setting, and participants: This was a single-institution, retrospective analysis in CRPC patients (N=119) who either received abiraterone before docetaxel (AD) (n=24) or did not receive abiraterone before docetaxel (docetaxel-only; n=95). Men initiated docetaxel between December 2007 (the date abiraterone was first used at our center) and May 2013.
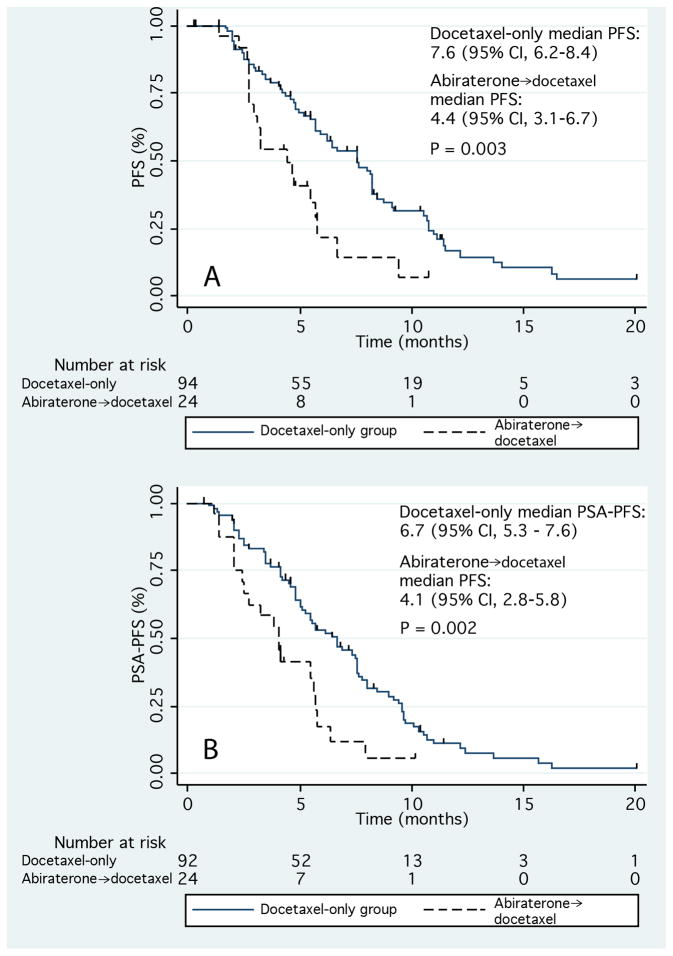
Outcome measurements and statistical analysis: The primary efficacy end points were prostate-specific antigen progression-free survival (PSA-PFS) and clinical/radiographic progression-free survival (PFS) on docetaxel. Differences between groups were assessed using univariate and multivariable analyses.
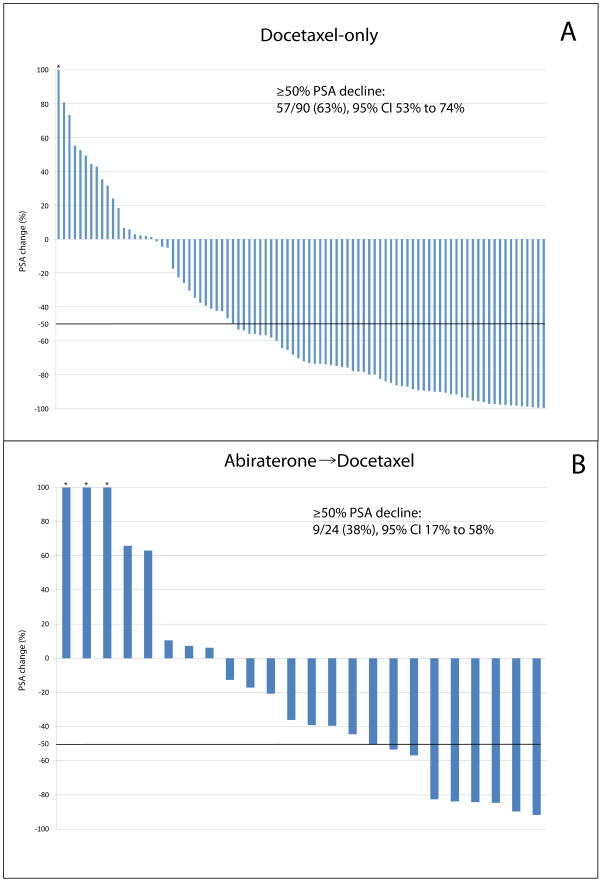
Results and limitations: Men in the AD group had a significantly higher risk for progression than those in the docetaxel-only group. Median PSA-PFS was 4.1 mo in the AD group and 6.7 mo in the docetaxel-only group (p=0.002). Median PFS was also shorter in the AD group (4.4 mo vs 7.6 mo; p=0.003). In multivariable analysis, prior abiraterone treatment remained an independent predictor of shorter PSA-PFS (hazard ratio [HR]: 3.48; 95% confidence interval [CI], 1.36-8.94; p=0.01) and PFS (HR: 3.62; 95% CI, 1.41-9.27; p=0.008). PSA declines ≥50% were less frequent in the AD group (38% vs 63%; p=0.02). The small size and retrospective nature of this study may have introduced bias.
Conclusions: Men receiving abiraterone before docetaxel were more likely to progress on docetaxel and less likely to achieve a PSA response than abiraterone-naïve patients. Cross-resistance between abiraterone and docetaxel may explain these findings; however, larger, more definitive studies are still needed to confirm this.
Patient summary: We examined the efficacy of docetaxel in castration-resistant prostate cancer patients who either did or did not receive prior abiraterone. We found that men receiving abiraterone before docetaxel were less likely to achieve a PSA response and were more likely to progress sooner on docetaxel than abiraterone-untreated patients. This may be due to cross-resistance.
Keywords: Abiraterone; Activity; Docetaxel; Efficacy; Progression-free survival; Prostate cancer.
Copyright © 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
One size does not fit all: can we choose the best sequence of treatment in asymptomatic castration-resistant prostate cancer patients?Eur Urol. 2014 Oct;66(4):653-4. doi: 10.1016/j.eururo.2014.03.024. Epub 2014 Mar 31. Eur Urol. 2014. PMID: 24735730 No abstract available.
-
Re: Michael T. Schweizer, Xian C. Zhou, Hao Wang, et al. The Influence of Prior Abiraterone Treatment on the Clinical Activity of Docetaxel in Men with Metastatic Castration-resistant Prostate Cancer. Eur Urol 2014;66:646-52.Eur Urol. 2015 Jun;67(6):e113-e114. doi: 10.1016/j.eururo.2014.12.018. Epub 2014 Dec 17. Eur Urol. 2015. PMID: 25534667 No abstract available.
Similar articles
-
Enzalutamide Antitumour Activity Against Metastatic Castration-resistant Prostate Cancer Previously Treated with Docetaxel and Abiraterone: A Multicentre Analysis.Eur Urol. 2015 Aug;68(2):317-24. doi: 10.1016/j.eururo.2014.07.028. Epub 2014 Aug 6. Eur Urol. 2015. PMID: 25108579
-
Androgen Receptor Splice Variant 7 and Efficacy of Taxane Chemotherapy in Patients With Metastatic Castration-Resistant Prostate Cancer.JAMA Oncol. 2015 Aug;1(5):582-91. doi: 10.1001/jamaoncol.2015.1341. JAMA Oncol. 2015. PMID: 26181238 Free PMC article.
-
Efficacy of enzalutamide following abiraterone acetate in chemotherapy-naive metastatic castration-resistant prostate cancer patients.Eur Urol. 2015 Jan;67(1):23-29. doi: 10.1016/j.eururo.2014.06.045. Epub 2014 Jul 10. Eur Urol. 2015. PMID: 25018038
-
Treating Patients with Metastatic Castration Resistant Prostate Cancer: A Comprehensive Review of Available Therapies.J Urol. 2015 Dec;194(6):1537-47. doi: 10.1016/j.juro.2015.06.106. Epub 2015 Jul 18. J Urol. 2015. PMID: 26196735 Review.
-
Docetaxel Activity in the Era of Life-prolonging Hormonal Therapies for Metastatic Castration-resistant Prostate Cancer.Eur Urol. 2016 Sep;70(3):410-2. doi: 10.1016/j.eururo.2016.05.002. Epub 2016 May 13. Eur Urol. 2016. PMID: 27184379 Review.
Cited by
-
Preclinical Models in Prostate Cancer: Resistance to AR Targeting Therapies in Prostate Cancer.Cancers (Basel). 2021 Feb 22;13(4):915. doi: 10.3390/cancers13040915. Cancers (Basel). 2021. PMID: 33671614 Free PMC article. Review.
-
Expert recommendations on the management of patients with metastatic castration-resistant prostate cancer who progress after CHAARTED or LATITUDE.Ther Adv Med Oncol. 2020 May 27;12:1758835920920067. doi: 10.1177/1758835920920067. eCollection 2020. Ther Adv Med Oncol. 2020. PMID: 33014145 Free PMC article.
-
Impact of taxanes on androgen receptor signaling.Asian J Androl. 2019 May-Jun;21(3):249-252. doi: 10.4103/aja.aja_37_18. Asian J Androl. 2019. PMID: 29900882 Free PMC article. Review.
-
Strategies to avoid treatment-induced lineage crisis in advanced prostate cancer.Nat Rev Clin Oncol. 2017 May;14(5):269-283. doi: 10.1038/nrclinonc.2016.181. Epub 2016 Nov 22. Nat Rev Clin Oncol. 2017. PMID: 27874061 Free PMC article. Review.
-
Targeting persistent androgen receptor signaling in castration-resistant prostate cancer.Med Oncol. 2016 May;33(5):44. doi: 10.1007/s12032-016-0759-3. Epub 2016 Apr 4. Med Oncol. 2016. PMID: 27042852 Review.
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Huggins C, Hodges CV. Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. 1941. J Urol. 2002;168:9–12. - PubMed
-
- Huggins C, Hodges CV. Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate 1941. J Urol. 2002;167:948–51. - PubMed
-
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
