

Impact of intermittent screening and treatment for malaria among school children in Kenya: a cluster randomised trial
- PMID: 24492859
- PMCID: PMC3904819
- DOI: 10.1371/journal.pmed.1001594
Impact of intermittent screening and treatment for malaria among school children in Kenya: a cluster randomised trial
Abstract
Background: Improving the health of school-aged children can yield substantial benefits for cognitive development and educational achievement. However, there is limited experimental evidence of the benefits of alternative school-based malaria interventions or how the impacts of interventions vary according to intensity of malaria transmission. We investigated the effect of intermittent screening and treatment (IST) for malaria on the health and education of school children in an area of low to moderate malaria transmission.
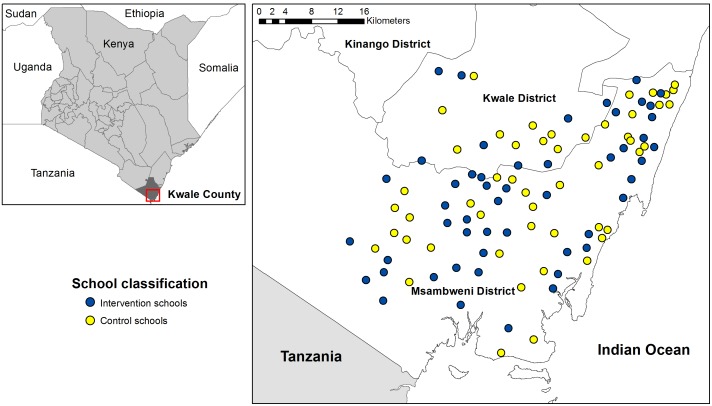
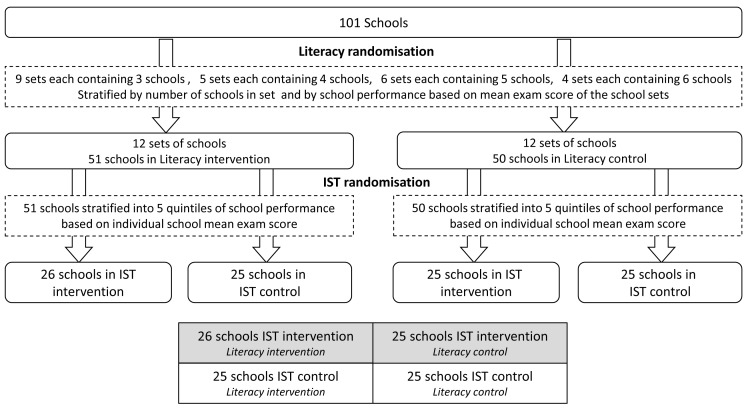
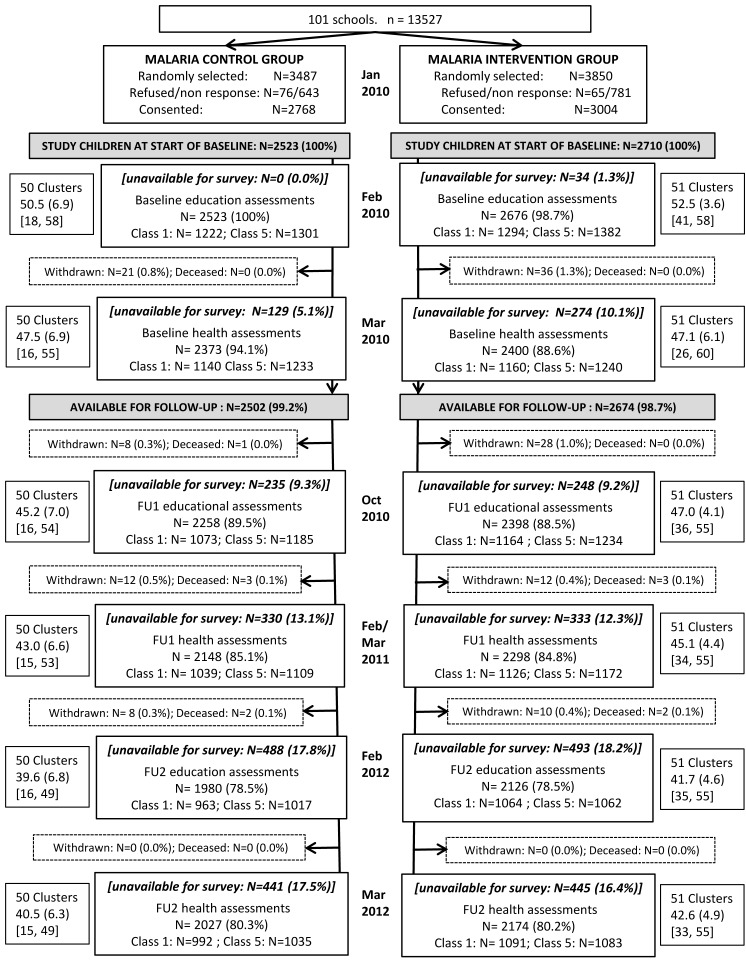
Methods and findings: A cluster randomised trial was implemented with 5,233 children in 101 government primary schools on the south coast of Kenya in 2010-2012. The intervention was delivered to children randomly selected from classes 1 and 5 who were followed up for 24 months. Once a school term, children were screened by public health workers using malaria rapid diagnostic tests (RDTs), and children (with or without malaria symptoms) found to be RDT-positive were treated with a six dose regimen of artemether-lumefantrine (AL). Given the nature of the intervention, the trial was not blinded. The primary outcomes were anaemia and sustained attention. Secondary outcomes were malaria parasitaemia and educational achievement. Data were analysed on an intention-to-treat basis. During the intervention period, an average of 88.3% children in intervention schools were screened at each round, of whom 17.5% were RDT-positive. 80.3% of children in the control and 80.2% in the intervention group were followed-up at 24 months. No impact of the malaria IST intervention was observed for prevalence of anaemia at either 12 or 24 months (adjusted risk ratio [Adj.RR]: 1.03, 95% CI 0.93-1.13, p = 0.621 and Adj.RR: 1.00, 95% CI 0.90-1.11, p = 0.953) respectively, or on prevalence of P. falciparum infection or scores of classroom attention. No effect of IST was observed on educational achievement in the older class, but an apparent negative effect was seen on spelling scores in the younger class at 9 and 24 months and on arithmetic scores at 24 months.
Conclusion: In this setting in Kenya, IST as implemented in this study is not effective in improving the health or education of school children. Possible reasons for the absence of an impact are the marked geographical heterogeneity in transmission, the rapid rate of reinfection following AL treatment, the variable reliability of RDTs, and the relative contribution of malaria to the aetiology of anaemia in this setting.
Trial registration: www.ClinicalTrials.gov NCT00878007.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
The failure of screening and treating as a malaria elimination strategy.PLoS Med. 2014 Jan 28;11(1):e1001595. doi: 10.1371/journal.pmed.1001595. eCollection 2014 Jan. PLoS Med. 2014. PMID: 24492211 Free PMC article.
Similar articles
-
Improving educational achievement and anaemia of school children: design of a cluster randomised trial of school-based malaria prevention and enhanced literacy instruction in Kenya.Trials. 2010 Oct 7;11:93. doi: 10.1186/1745-6215-11-93. Trials. 2010. PMID: 20929566 Free PMC article. Clinical Trial.
-
Plasmodium falciparum, anaemia and cognitive and educational performance among school children in an area of moderate malaria transmission: baseline results of a cluster randomized trial on the coast of Kenya.Trop Med Int Health. 2012 May;17(5):532-49. doi: 10.1111/j.1365-3156.2012.02971.x. Trop Med Int Health. 2012. PMID: 22950512 Free PMC article. Clinical Trial.
-
Effect of intermittent preventive treatment of malaria on health and education in schoolchildren: a cluster-randomised, double-blind, placebo-controlled trial.Lancet. 2008 Jul 12;372(9633):127-138. doi: 10.1016/S0140-6736(08)61034-X. Lancet. 2008. PMID: 18620950 Free PMC article. Clinical Trial.
-
Preventive malaria treatment among school-aged children in sub-Saharan Africa: a systematic review and meta-analyses.Lancet Glob Health. 2020 Dec;8(12):e1499-e1511. doi: 10.1016/S2214-109X(20)30325-9. Epub 2020 Oct 22. Lancet Glob Health. 2020. PMID: 33222799 Free PMC article.
-
Impact of Plasmodium falciparum malaria and intermittent preventive treatment of malaria in pregnancy on the risk of malaria in infants: a systematic review.Malar J. 2019 Sep 3;18(1):304. doi: 10.1186/s12936-019-2943-3. Malar J. 2019. PMID: 31481075 Free PMC article.
Cited by
-
Field performance of ultrasensitive and conventional malaria rapid diagnostic tests in southern Mozambique.Malar J. 2020 Dec 7;19(1):451. doi: 10.1186/s12936-020-03526-9. Malar J. 2020. PMID: 33287822 Free PMC article.
-
Comparing insecticide-treated bed net use to Plasmodium falciparum infection among schoolchildren living near Lake Victoria, Kenya.Malar J. 2015 Dec 22;14:515. doi: 10.1186/s12936-015-1031-6. Malar J. 2015. PMID: 26696416 Free PMC article.
-
Impact of Community-Based Mass Testing and Treatment on Malaria Infection Prevalence in a High-Transmission Area of Western Kenya: A Cluster Randomized Controlled Trial.Clin Infect Dis. 2021 Jun 1;72(11):1927-1935. doi: 10.1093/cid/ciaa471. Clin Infect Dis. 2021. PMID: 32324850 Free PMC article. Clinical Trial.
-
Intermittent screening and treatment for malaria complementary to routine immunisation in the first year of life in Papua, Indonesia: a cluster randomised superiority trial.BMC Med. 2022 Jun 8;20(1):190. doi: 10.1186/s12916-022-02394-1. BMC Med. 2022. PMID: 35672703 Free PMC article. Clinical Trial.
-
It Is Time to Strengthen the Malaria Control Policy of the Democratic Republic of Congo and Include Schools and School-Age Children in Malaria Control Measures.Pathogens. 2022 Jun 26;11(7):729. doi: 10.3390/pathogens11070729. Pathogens. 2022. PMID: 35889975 Free PMC article. Review.
References
-
- O'Meara WP, Mangeni JN, Steketee R, Greenwood B (2010) Changes in the burden of malaria in sub-Saharan Africa. Lancet Infect Dis 10: 545–555. - PubMed
-
- Ceesay SJ, Casals-Pascual C, Nwakanma DC, Walther M, Gomez-Escobar N, et al. (2010) Continued decline of malaria in The Gambia with implications for elimination. PLoS ONE 5: e12242 doi:10.1371/journal.pone.0012242 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
