

Specialty use among patients with treated hypertension in a patient-centered medical home
- PMID: 24493321
- PMCID: PMC4000327
- DOI: 10.1007/s11606-014-2776-2
Specialty use among patients with treated hypertension in a patient-centered medical home
Abstract
Background: Little is known about how delivery of primary care in the patient-centered medical home (PCMH) influences outpatient specialty care use.
Objective: To describe changes in outpatient specialty use among patients with treated hypertension during and after PCMH practice transformation.
Design: One-group, 48-month interrupted time series across baseline, PCMH implementation and post-implementation periods.
Patients: Adults aged 18-85 years with treated hypertension.
Intervention: System-wide PCMH redesign implemented across 26 clinics in an integrated health care delivery system, beginning in January 2009.
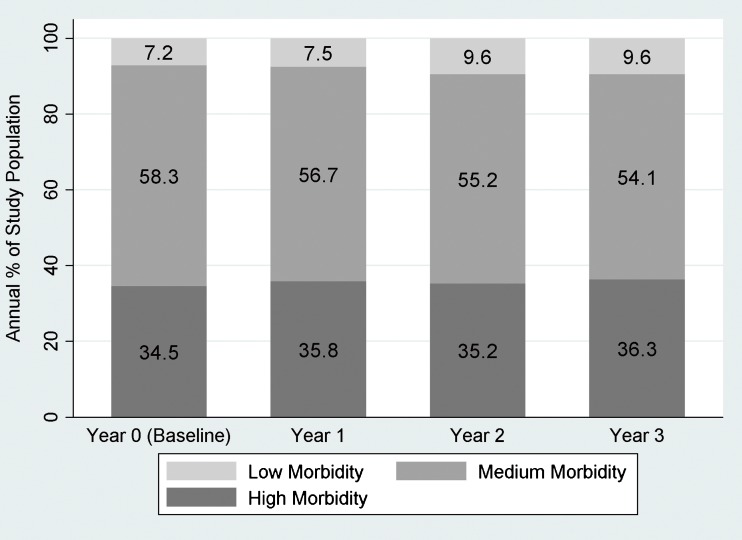
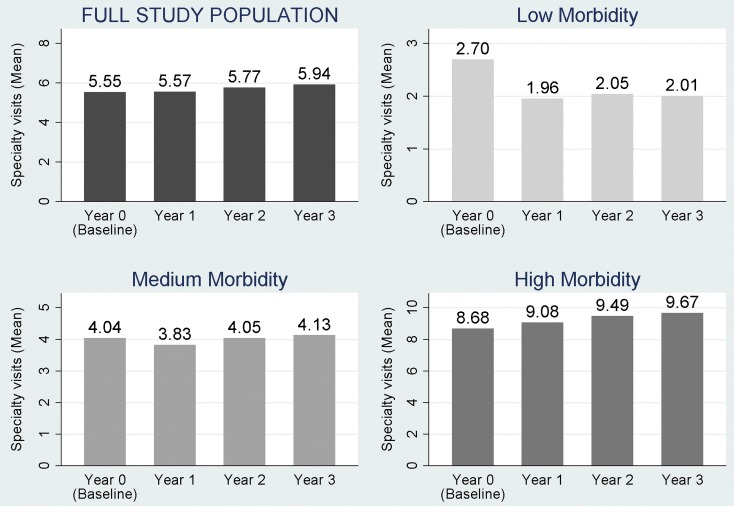
Main measures: Resource Utilization Band variables from the Adjusted Clinical Groups case mix software characterized overall morbidity burden (low, medium, high). Negative binomial regression models described adjusted annual differences in total specialty care visits. Poisson regression models described adjusted annual differences in any use (yes/no) of selected medical and surgical specialties.
Key results: Compared to baseline, the study population averaged 7% fewer adjusted specialty visits during implementation (P < 0.001) and 4% fewer adjusted specialty visits in the first post-implementation year (P = 0.02). Patients were 12% less likely to have any cardiology visits during implementation and 13% less likely during the first post-implementation year (P < 0.001). In interaction analysis, patients with low morbidity had at least 27% fewer specialty visits during each of 3 years following baseline (P < 0.001); medium morbidity patients had 9% fewer specialty visits during implementation (P < 0.001) and 5% fewer specialty visits during the first post-implementation year (P = 0.007); high morbidity patients had 3% (P = 0.05) and 5% (P = 0.009) higher specialty use during the first and second post-implementation years, respectively.
Conclusions: Results suggest that more comprehensive primary care in this PCMH redesign enabled primary care teams to deliver more hypertension care, and that many needs of low morbidity patients were within the scope of primary care practice. New approaches to care coordination between primary care teams and specialists should prioritize high morbidity, clinically complex patients.
Figures
Comment in
-
Capsule commentary on Liss et al., Specialty use among patients with treated hypertension in a patient-centered medical home.J Gen Intern Med. 2014 May;29(5):786. doi: 10.1007/s11606-014-2824-y. J Gen Intern Med. 2014. PMID: 24647723 Free PMC article. No abstract available.
Similar articles
-
Patient-Centered Medical Home Implementation in the Veterans Health Administration and Primary Care Use: Differences by Patient Comorbidity Burden.J Gen Intern Med. 2016 Dec;31(12):1467-1474. doi: 10.1007/s11606-016-3833-9. Epub 2016 Aug 8. J Gen Intern Med. 2016. PMID: 27503440 Free PMC article.
-
Association of High-Cost Health Care Utilization With Longitudinal Changes in Patient-Centered Medical Home Implementation.JAMA Netw Open. 2020 Feb 5;3(2):e1920500. doi: 10.1001/jamanetworkopen.2019.20500. JAMA Netw Open. 2020. PMID: 32022880
-
Delivering PACT-principled care: are specialty care patients being left behind?J Gen Intern Med. 2014 Jul;29 Suppl 2(Suppl 2):S695-702. doi: 10.1007/s11606-013-2677-9. J Gen Intern Med. 2014. PMID: 24715390 Free PMC article.
-
Early changes in VA medical home components and utilization.Am J Manag Care. 2015 Mar;21(3):197-204. Am J Manag Care. 2015. PMID: 25880624
-
Outcomes among chronically ill adults in a medical home prototype.Am J Manag Care. 2013 Oct 1;19(10):e348-58. Am J Manag Care. 2013. PMID: 24304182 Free PMC article.
Cited by
-
Preparing Trainees to Deliver Patient-Centered Care in an Ambulatory Cancer Clinic.J Cancer Educ. 2015 Sep;30(3):460-5. doi: 10.1007/s13187-014-0719-6. J Cancer Educ. 2015. PMID: 25189797
-
Coordination of care in health systems for users with diabetes and hypertension: a scoping review.Rev Lat Am Enfermagem. 2025 Jan 27;33:e4428. doi: 10.1590/1518-8345.7198.4428. eCollection 2025. Rev Lat Am Enfermagem. 2025. PMID: 39879481 Free PMC article.
-
Capsule commentary on Liss et al., Specialty use among patients with treated hypertension in a patient-centered medical home.J Gen Intern Med. 2014 May;29(5):786. doi: 10.1007/s11606-014-2824-y. J Gen Intern Med. 2014. PMID: 24647723 Free PMC article. No abstract available.
References
-
- American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, American Osteopathic Association. Joint principles of the patient-centered medical home. 2007; http://www.aafp.org/dam/AAFP/documents/practice_management/pcmh/initiati.... Accessed January 10, 2014.
-
- Peikes D, Zutshi A, Genevro JL, Parchman ML, Meyers DS. Early evaluations of the medical home: building on a promising start. Am J Manag Care. 2012;18(2):105–116. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
