

Cytogenetic prognostication within medulloblastoma subgroups
- PMID: 24493713
- PMCID: PMC3948094
- DOI: 10.1200/JCO.2013.50.9539
Cytogenetic prognostication within medulloblastoma subgroups
Abstract
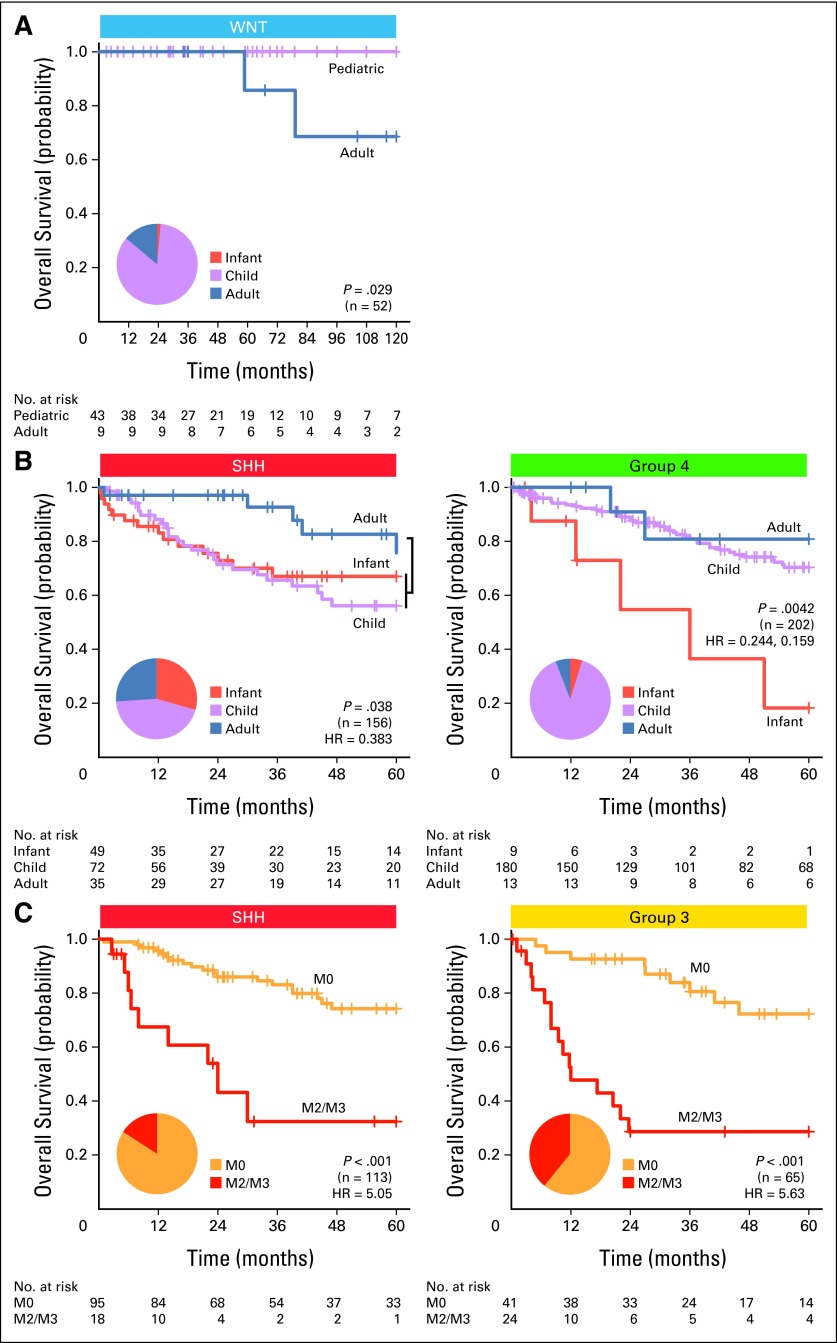
Purpose: Medulloblastoma comprises four distinct molecular subgroups: WNT, SHH, Group 3, and Group 4. Current medulloblastoma protocols stratify patients based on clinical features: patient age, metastatic stage, extent of resection, and histologic variant. Stark prognostic and genetic differences among the four subgroups suggest that subgroup-specific molecular biomarkers could improve patient prognostication.
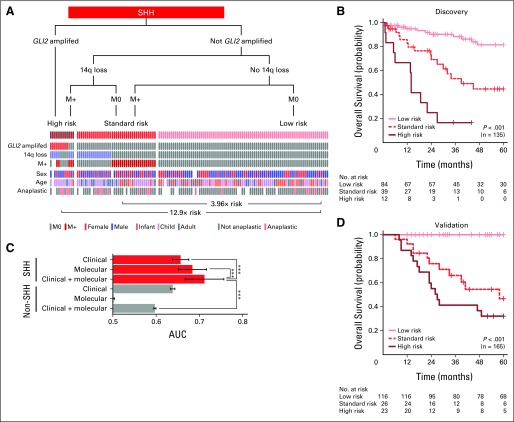
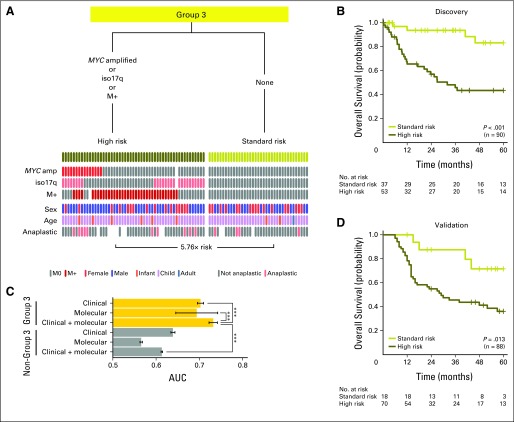
Patients and methods: Molecular biomarkers were identified from a discovery set of 673 medulloblastomas from 43 cities around the world. Combined risk stratification models were designed based on clinical and cytogenetic biomarkers identified by multivariable Cox proportional hazards analyses. Identified biomarkers were tested using fluorescent in situ hybridization (FISH) on a nonoverlapping medulloblastoma tissue microarray (n = 453), with subsequent validation of the risk stratification models.
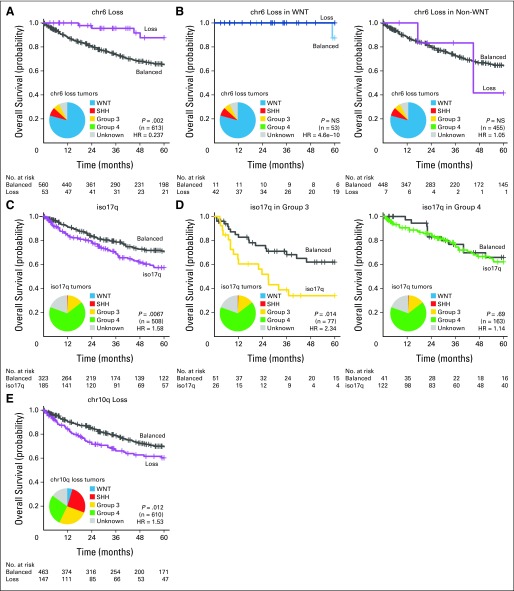
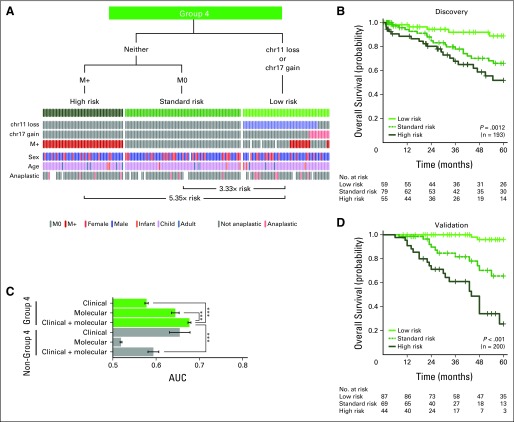
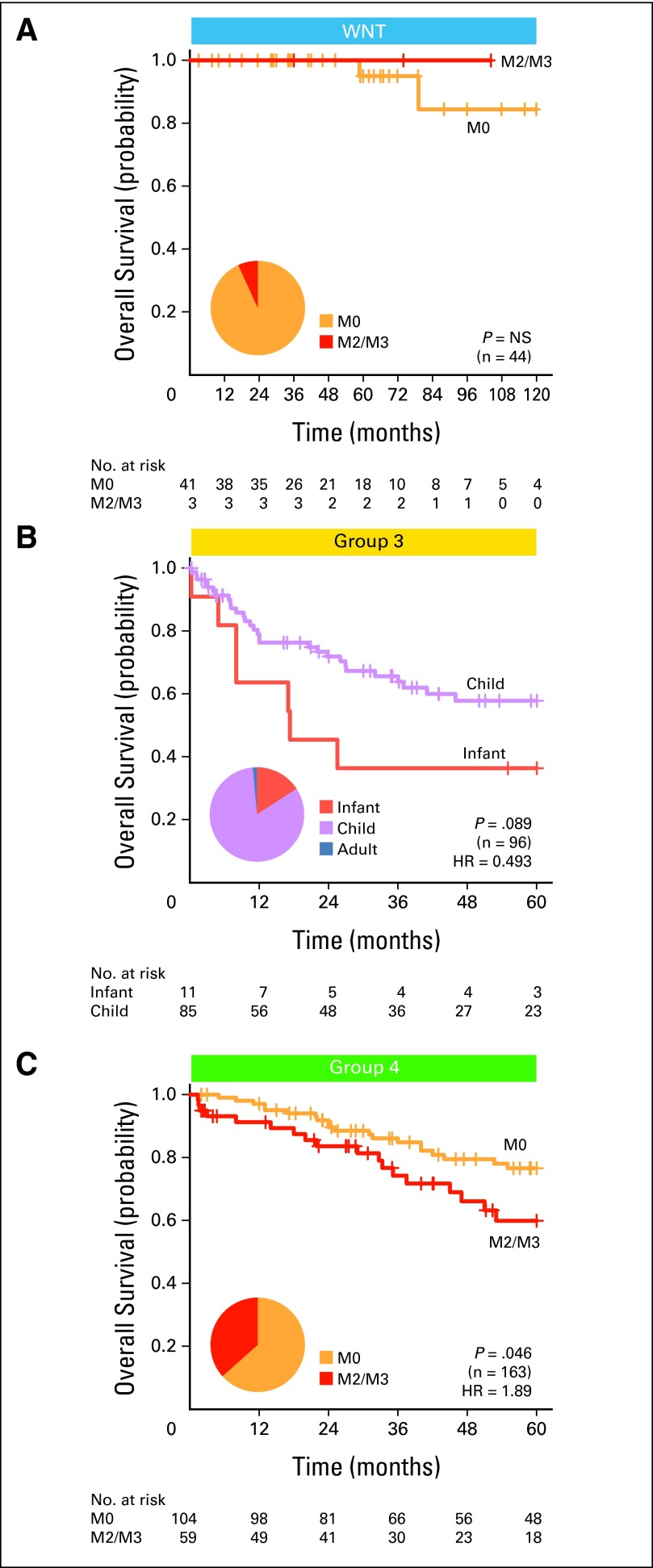
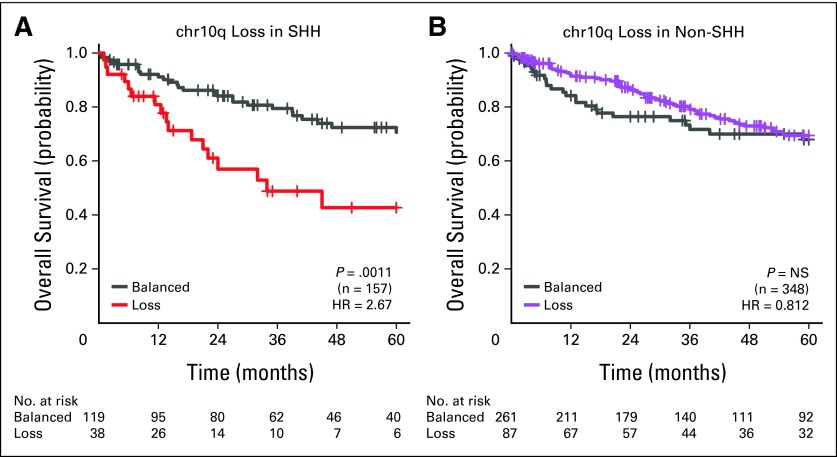
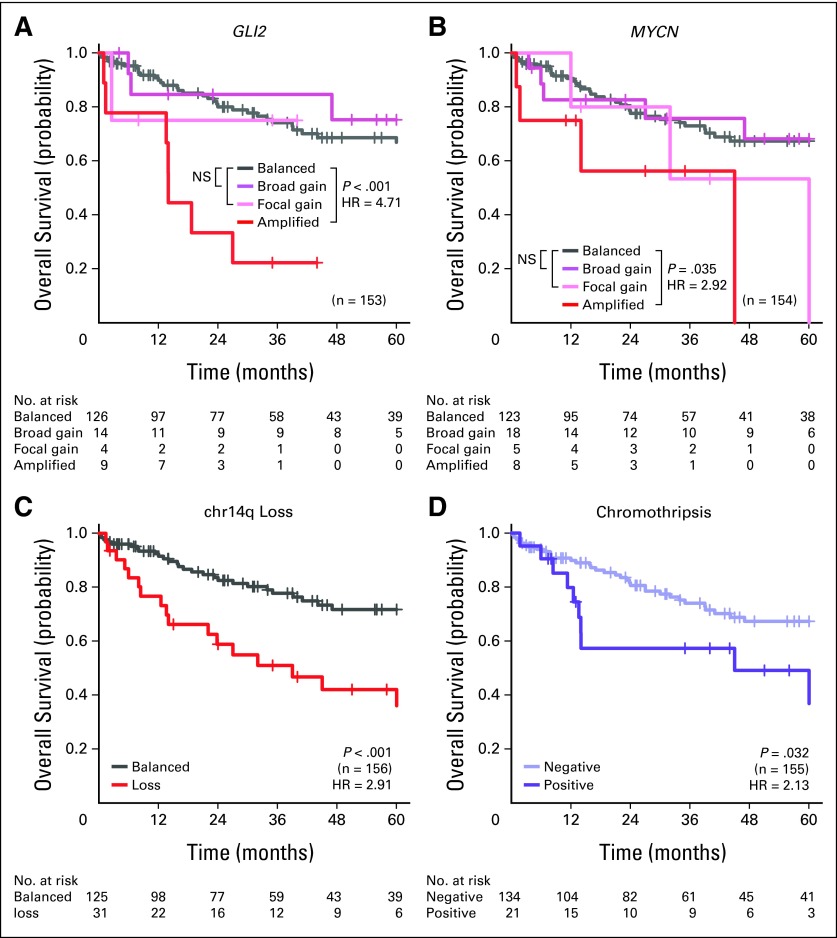
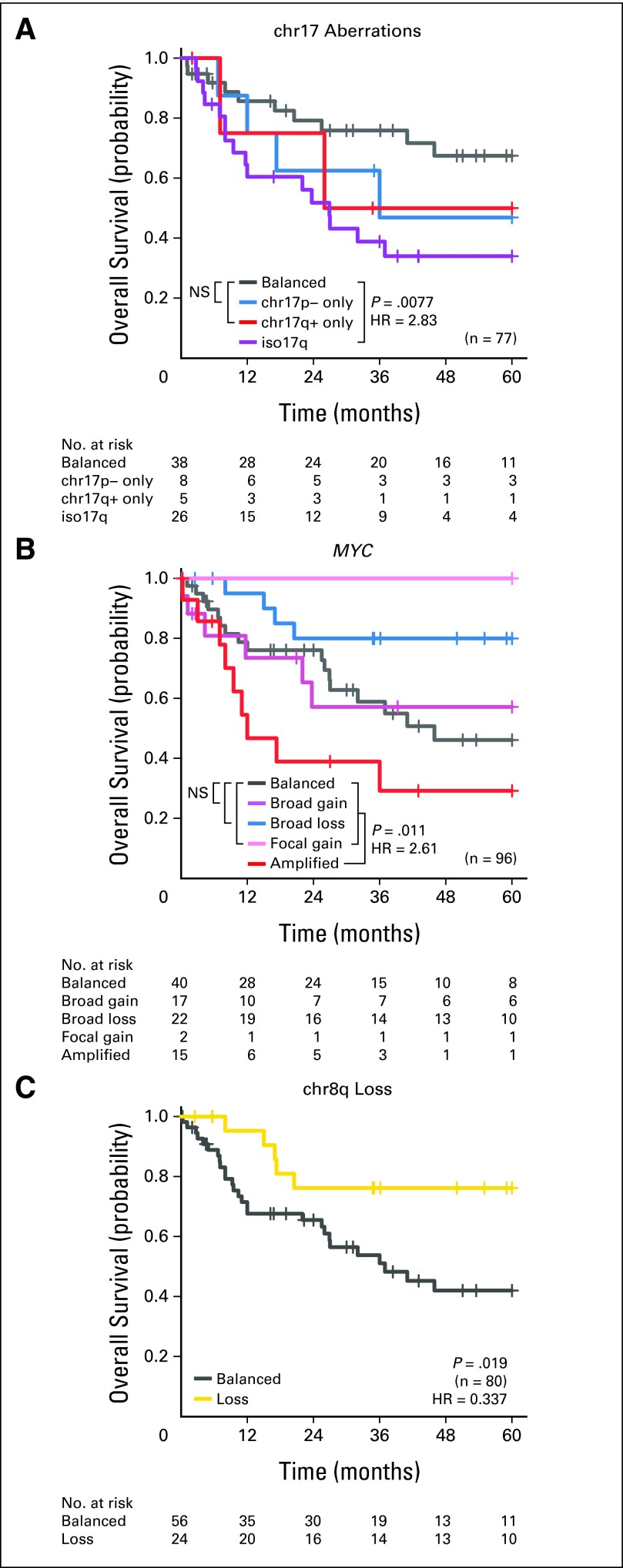
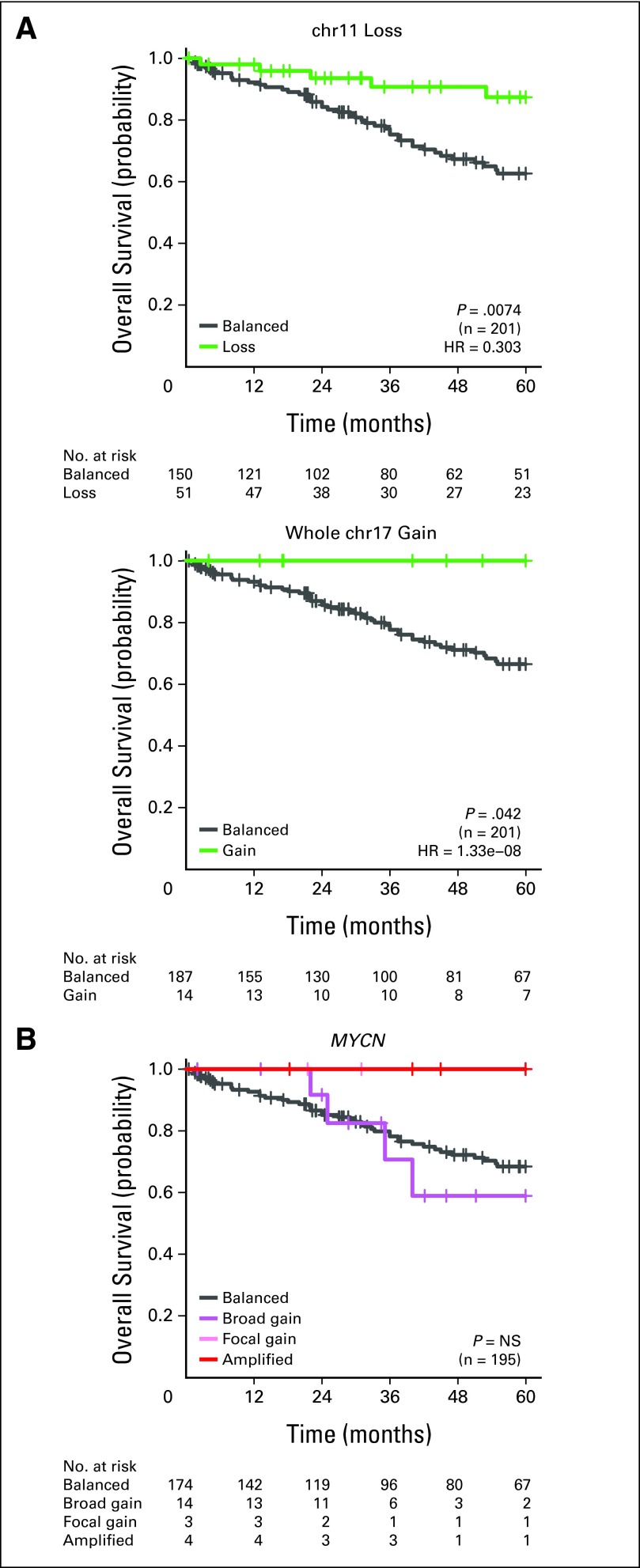
Results: Subgroup information improves the predictive accuracy of a multivariable survival model compared with clinical biomarkers alone. Most previously published cytogenetic biomarkers are only prognostic within a single medulloblastoma subgroup. Profiling six FISH biomarkers (GLI2, MYC, chromosome 11 [chr11], chr14, 17p, and 17q) on formalin-fixed paraffin-embedded tissues, we can reliably and reproducibly identify very low-risk and very high-risk patients within SHH, Group 3, and Group 4 medulloblastomas.
Conclusion: Combining subgroup and cytogenetic biomarkers with established clinical biomarkers substantially improves patient prognostication, even in the context of heterogeneous clinical therapies. The prognostic significance of most molecular biomarkers is restricted to a specific subgroup. We have identified a small panel of cytogenetic biomarkers that reliably identifies very high-risk and very low-risk groups of patients, making it an excellent tool for selecting patients for therapy intensification and therapy de-escalation in future clinical trials.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Gajjar A, Chintagumpala M, Ashley D, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): Long-term results from a prospective, multicentre trial. Lancet Oncol. 2006;7:813–820. - PubMed
-
- Northcott PA, Korshunov A, Pfister SM, et al. The clinical implications of medulloblastoma subgroups. Nat Rev Neurol. 2012;8:340–351. - PubMed
-
- Lannering B, Rutkowski S, Doz F, et al. Hyperfractionated versus conventional radiotherapy followed by chemotherapy in standard-risk medulloblastoma: Results from the randomized multicenter HIT-SIOP PNET 4 trial. J Clin Oncol. 2012;30:3187–3193. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
