

Clinical issues of mucus accumulation in COPD
- PMID: 24493923
- PMCID: PMC3908831
- DOI: 10.2147/COPD.S38938
Clinical issues of mucus accumulation in COPD
Abstract
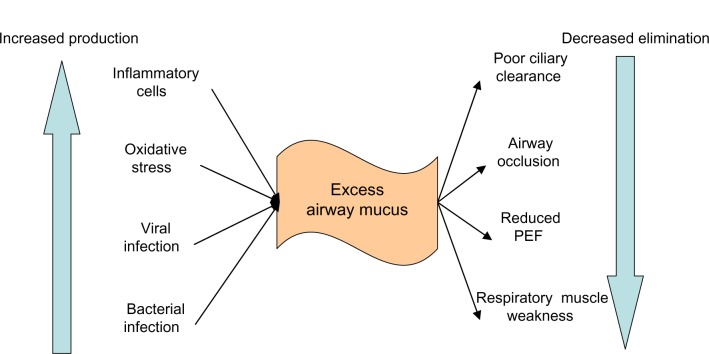
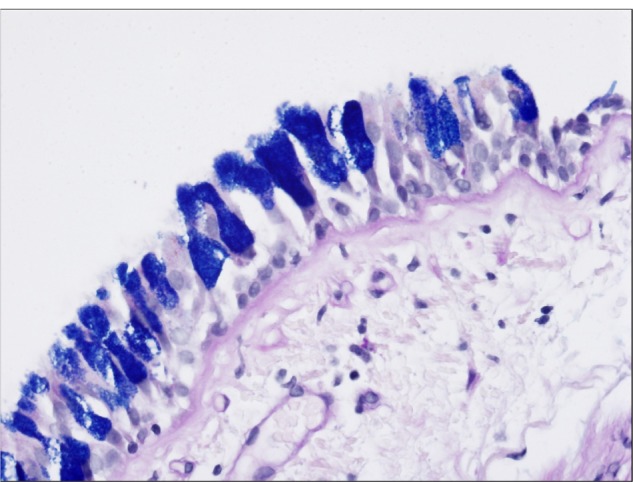
Airway mucus is part of the lung's native immune function that traps particulates and microorganisms, enabling their clearance from the lung by ciliary transport and cough. Mucus hypersecretion and chronic productive cough are the features of the chronic bronchitis and chronic obstructive pulmonary disease (COPD). Overproduction and hypersecretion by goblet cells and the decreased elimination of mucus are the primary mechanisms responsible for excessive mucus in chronic bronchitis. Mucus accumulation in COPD patients affects several important outcomes such as lung function, health-related quality of life, COPD exacerbations, hospitalizations, and mortality. Nonpharmacologic options for the treatment of mucus accumulation in COPD are smoking cessation and physical measures used to promote mucus clearance. Pharmacologic therapies include expectorants, mucolytics, methylxanthines, beta-adrenergic receptor agonists, anticholinergics, glucocorticoids, phosphodiesterase-4 inhibitors, antioxidants, and antibiotics.
Keywords: chronic bronchitis; chronic obstructive pulmonary disease; mucus; sputum.
Figures

Comment in
-
Clinical issues of mucus accumulation in COPD.Int J Chron Obstruct Pulmon Dis. 2014 Mar 25;9:301-2. doi: 10.2147/COPD.S61797. eCollection 2014. Int J Chron Obstruct Pulmon Dis. 2014. PMID: 24741301 Free PMC article. No abstract available.
References
-
- Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. - PubMed
-
- World Health Organization . World Health Statistics 2008. Geneva, Switzerland: World Health Organization; 2008. [Accessed July 23, 2013]. Available from: http://www.who.int/whosis/whostat/EN_WHS08_Full.pdf.
-
- Voynow JA, Rubin BK. Mucins, mucus, and sputum. Chest. 2009;135(2):505–512. - PubMed
-
- Shade D, Jr, Cordova FC. Normal lung structure. In: Criner GJ, D’Alonzo GE, editors. Pulmonary Pathophysiology. 1st ed. 1999. p. 20.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
