

Sunlight and Vitamin D: A global perspective for health
- PMID: 24494042
- PMCID: PMC3897598
- DOI: 10.4161/derm.24494
Sunlight and Vitamin D: A global perspective for health
Abstract
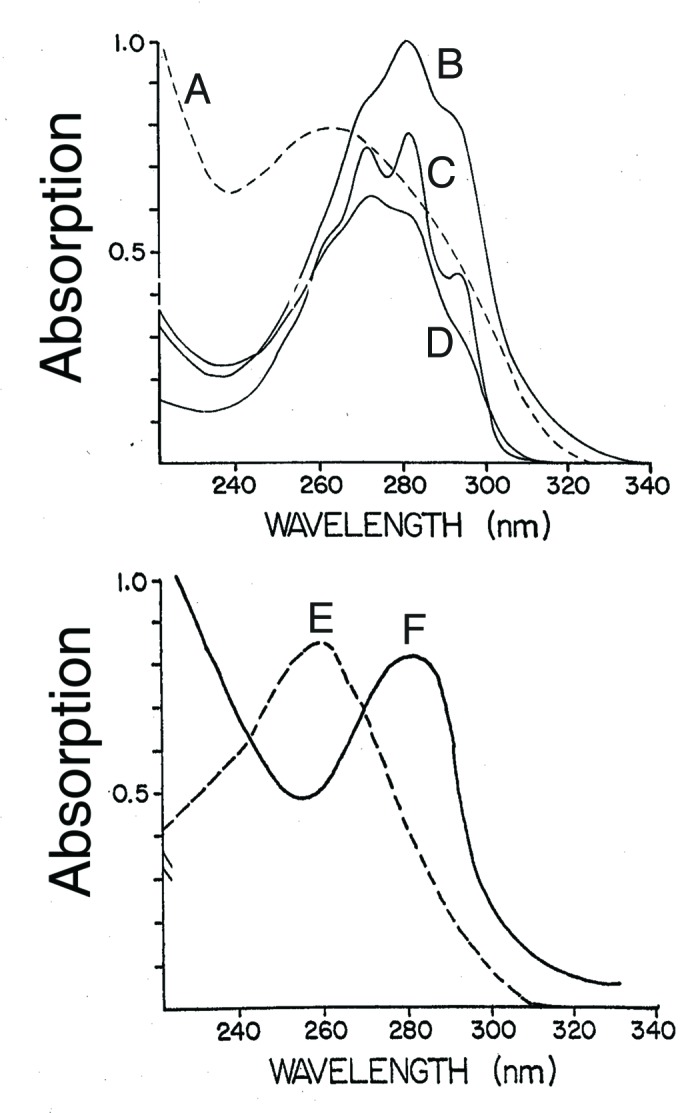
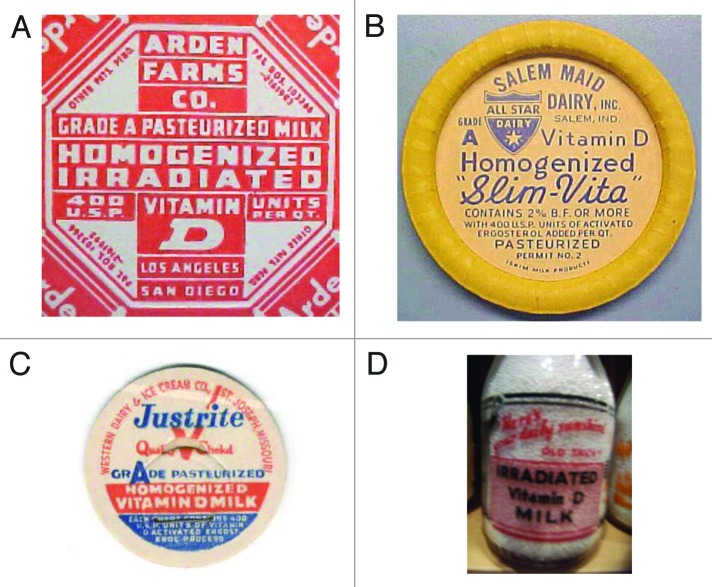
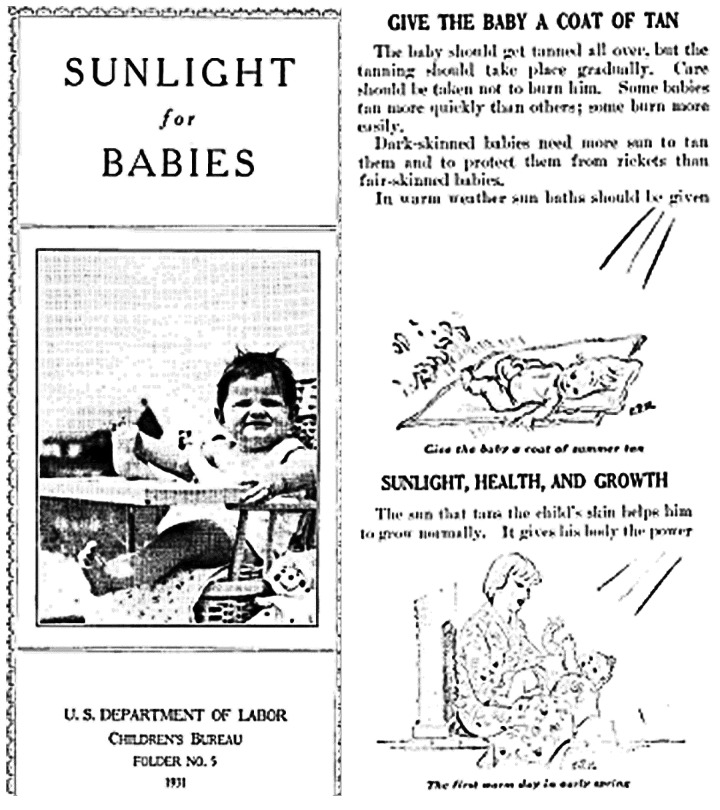
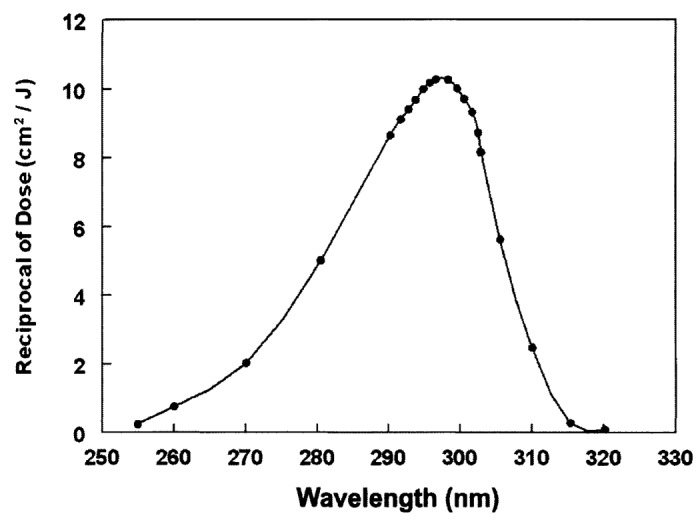
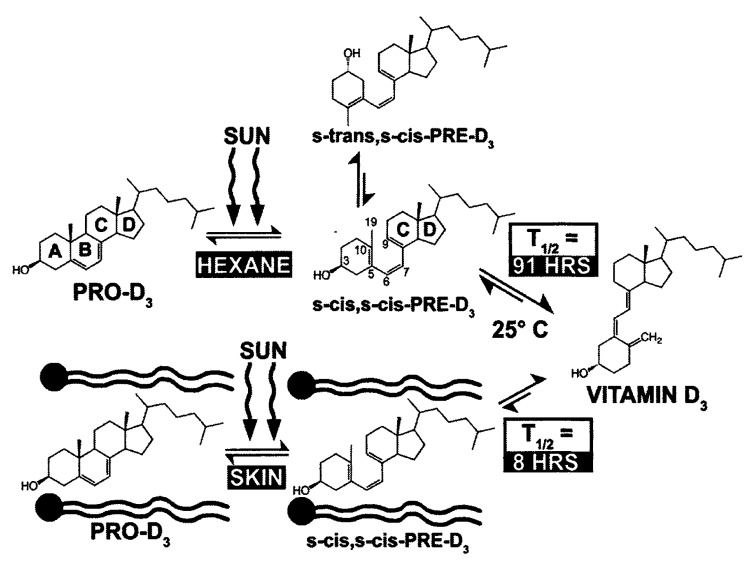
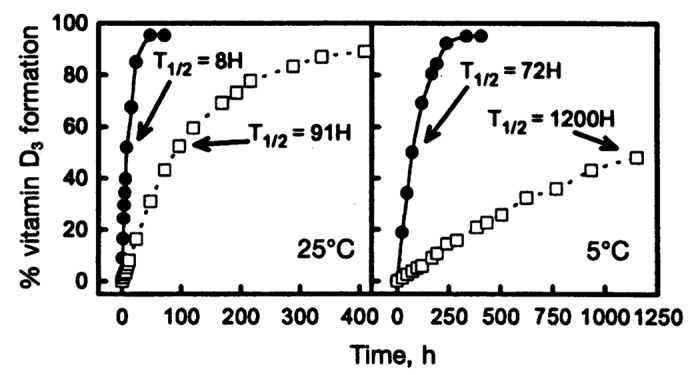
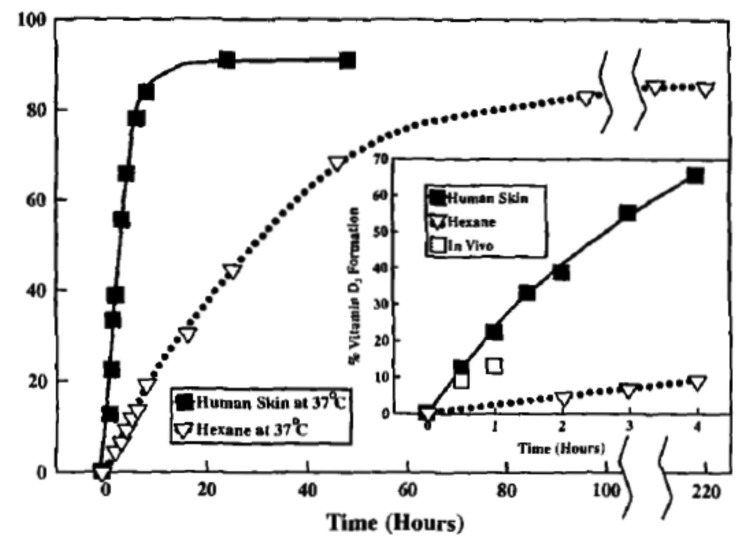
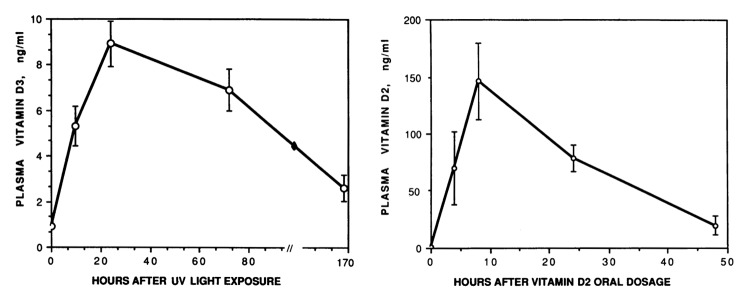
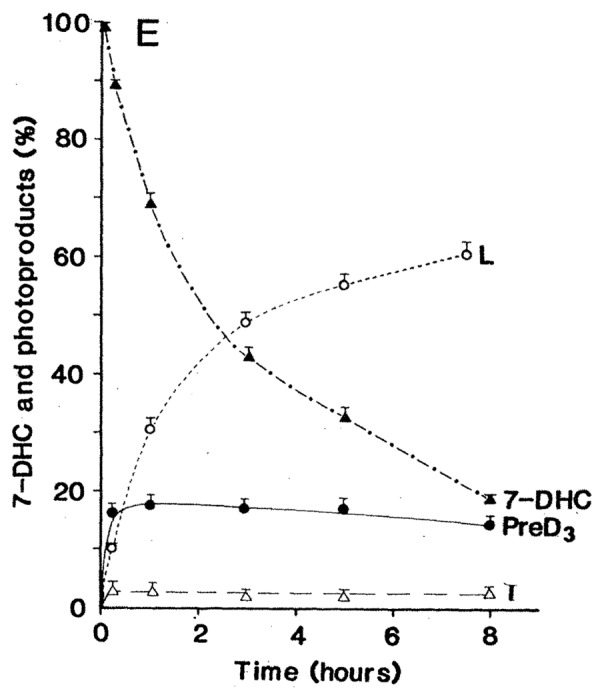
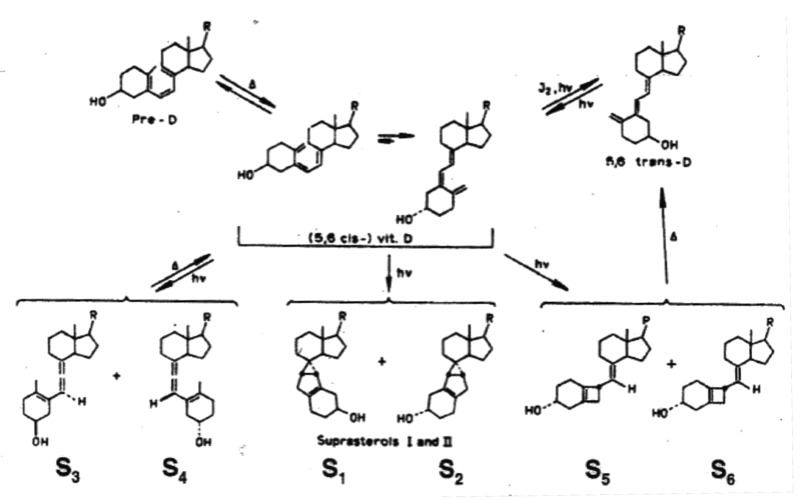
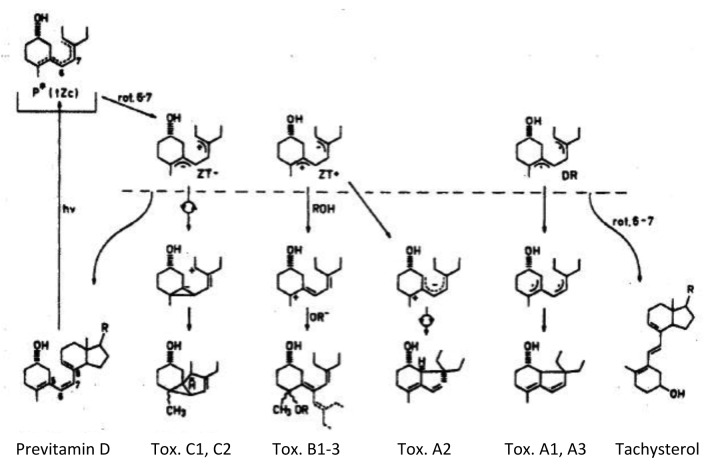
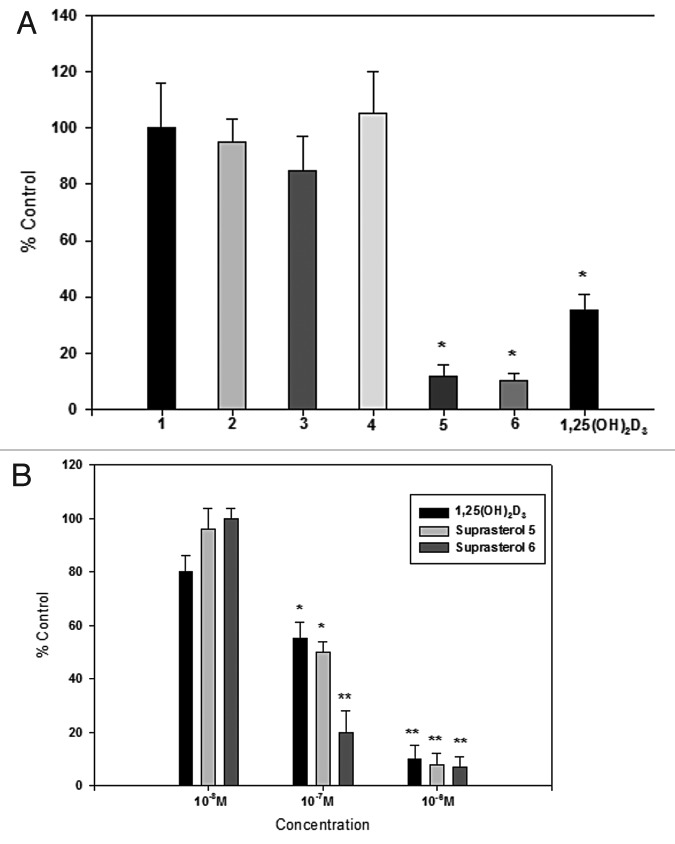
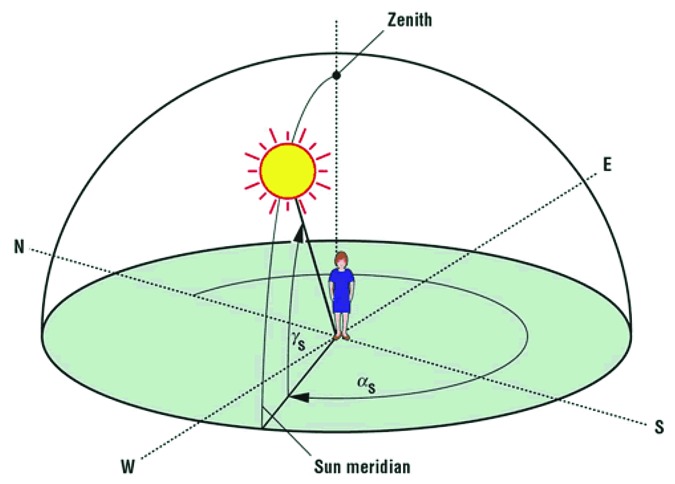
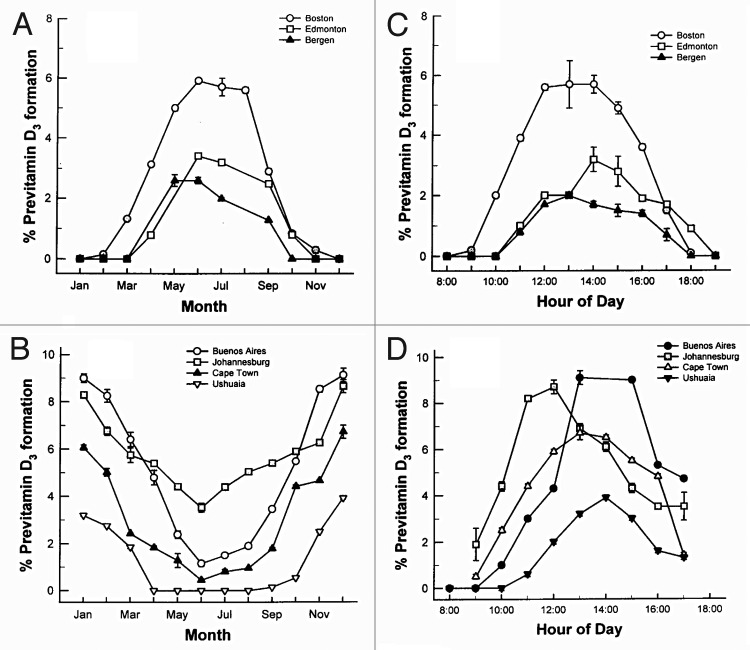
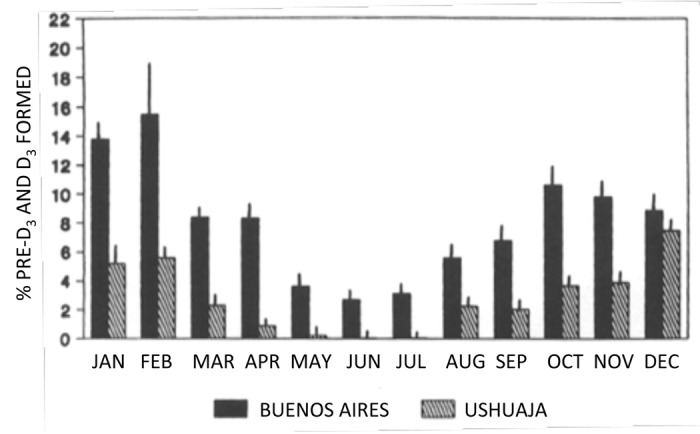
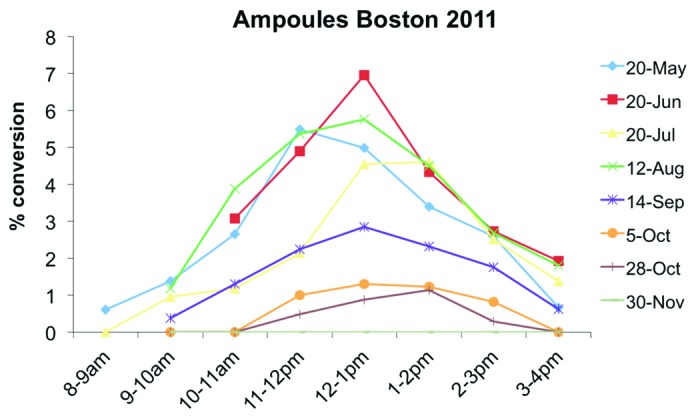
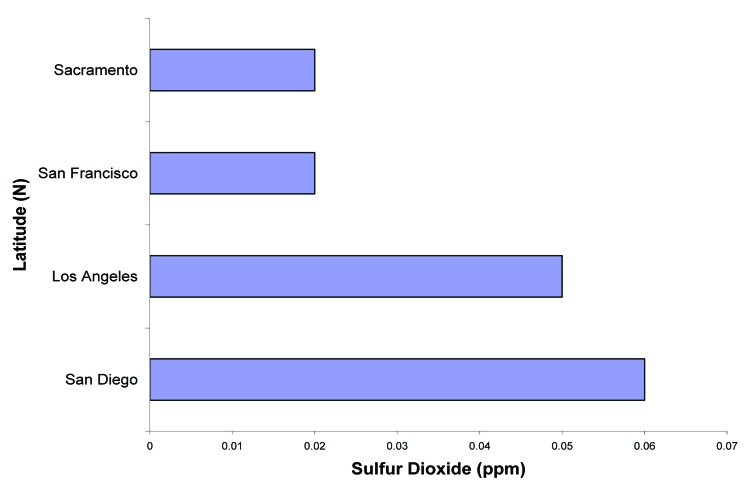
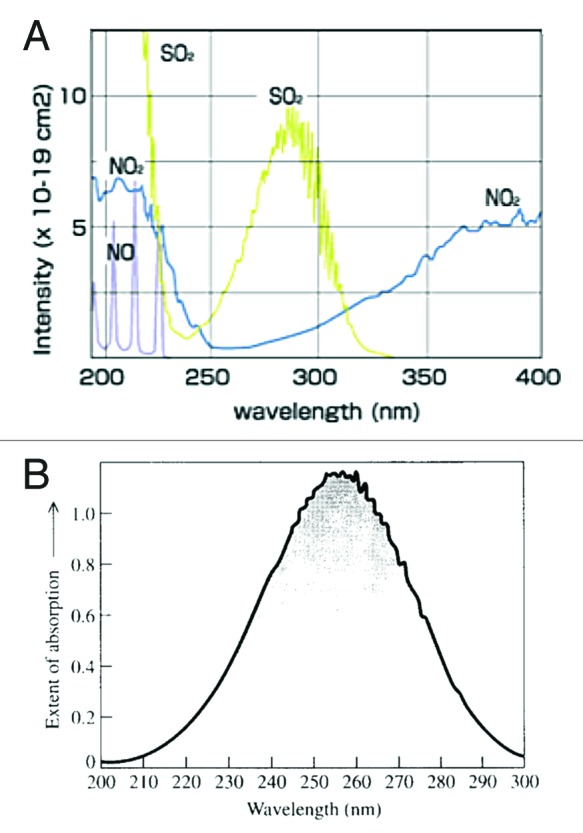
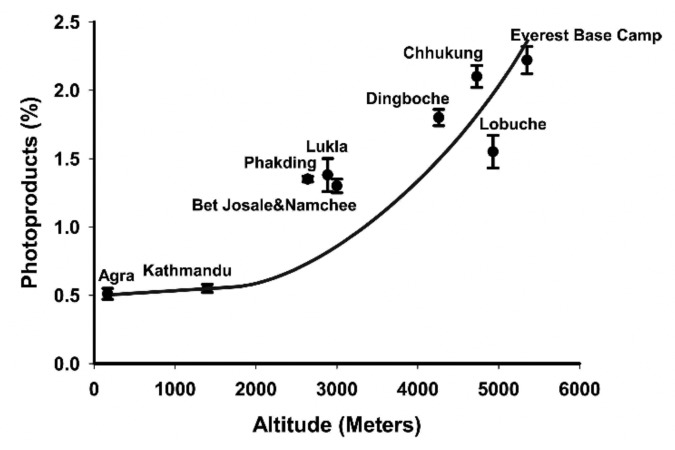
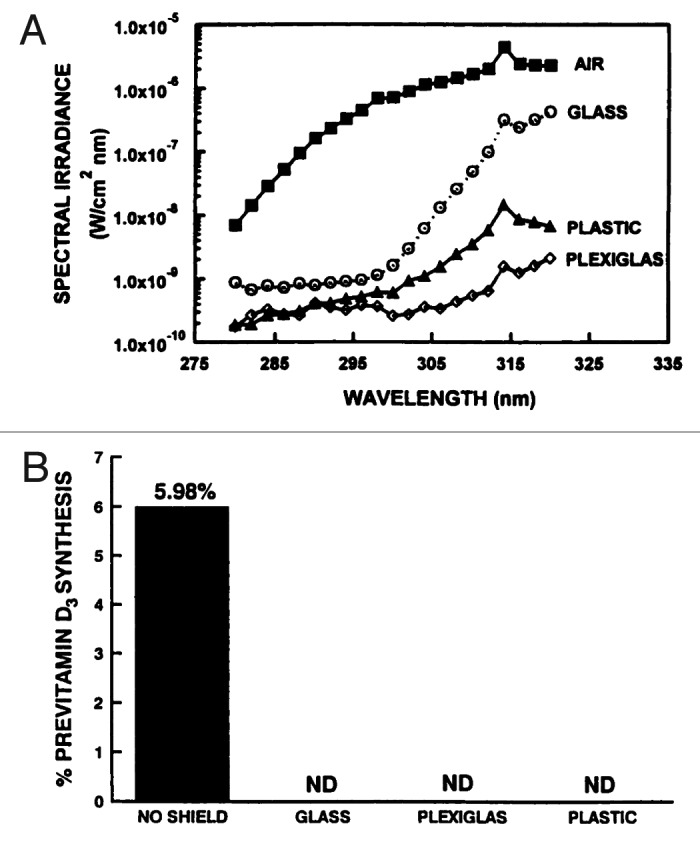
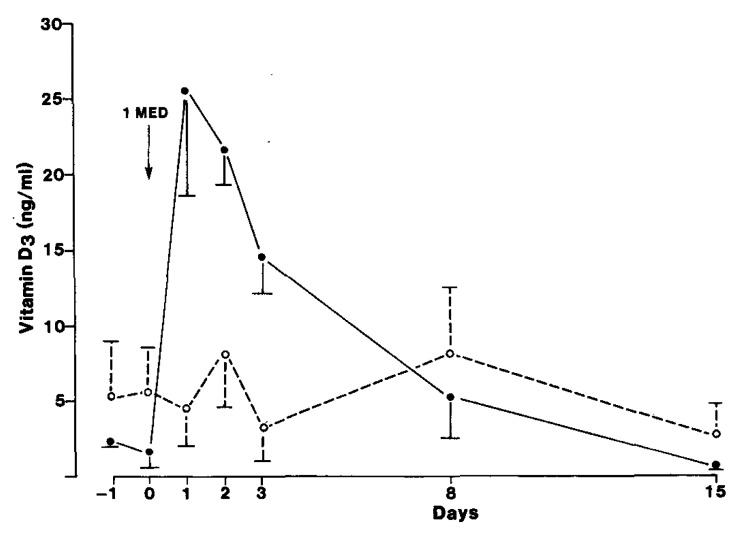
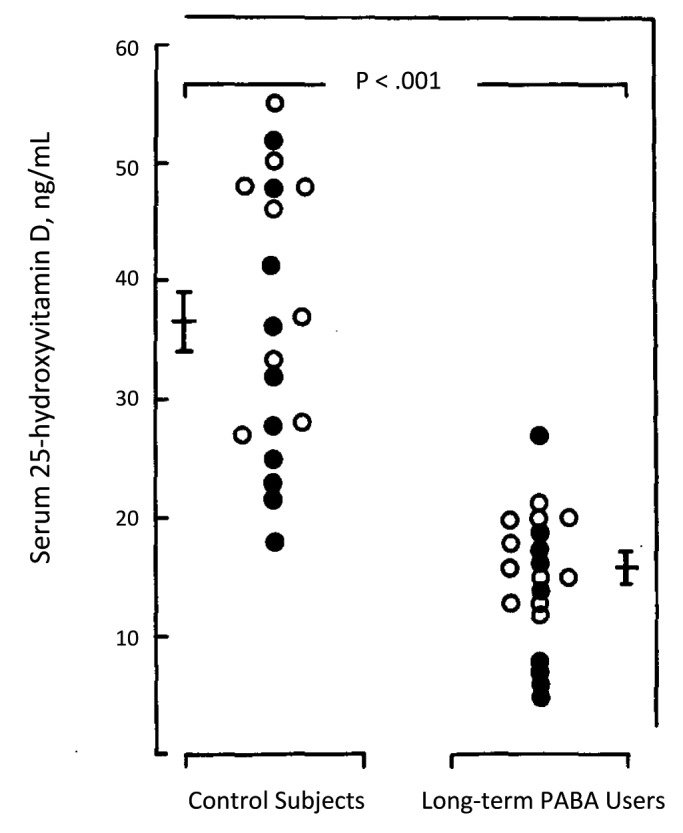
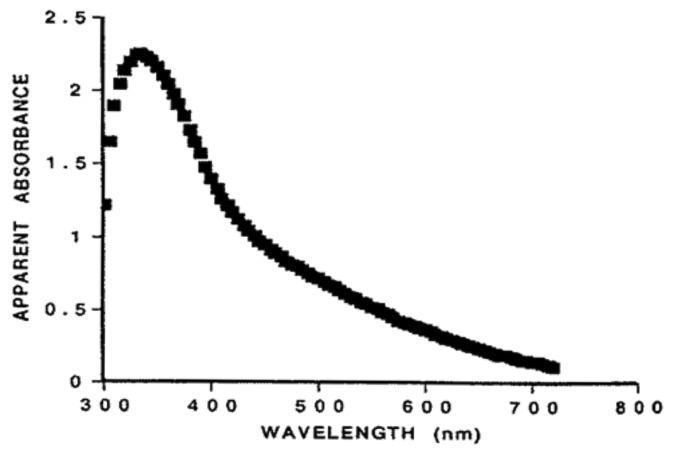
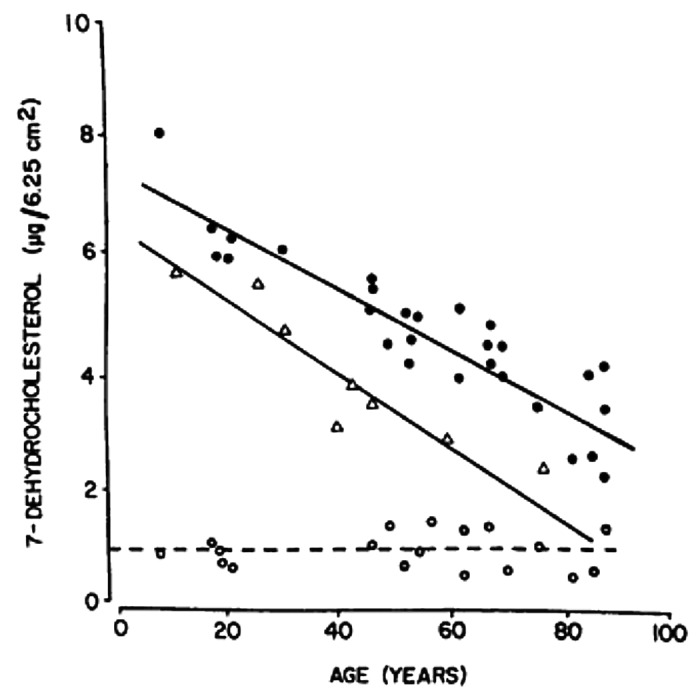
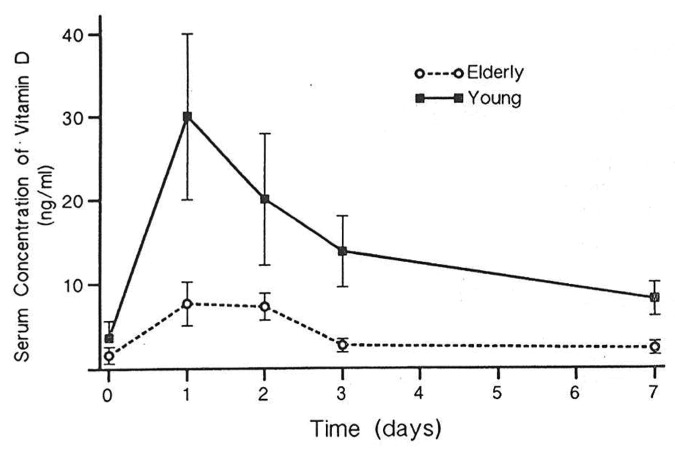
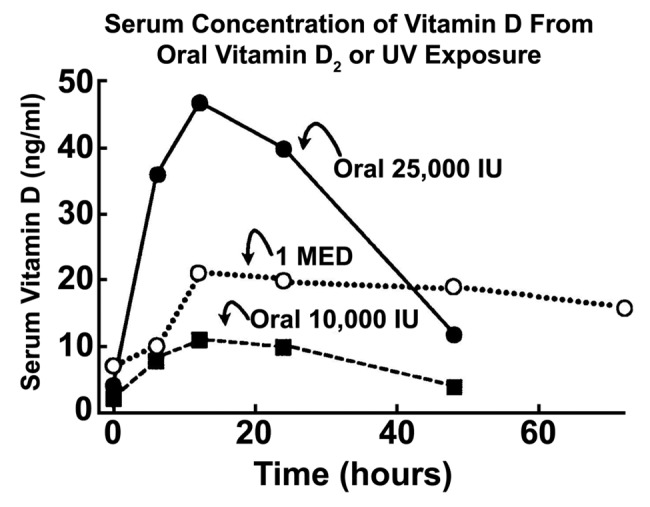
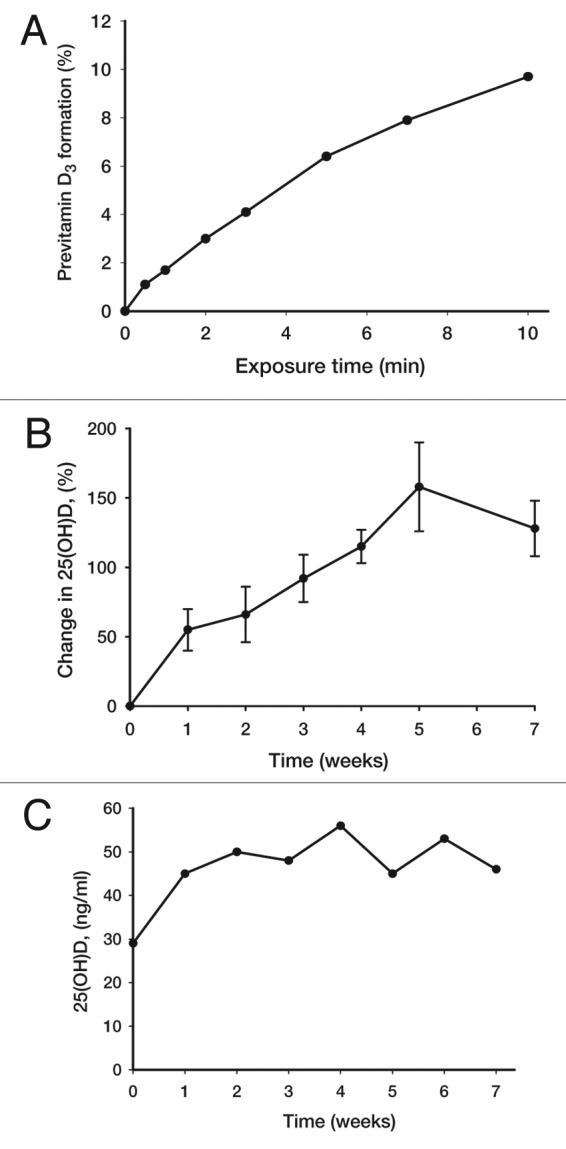
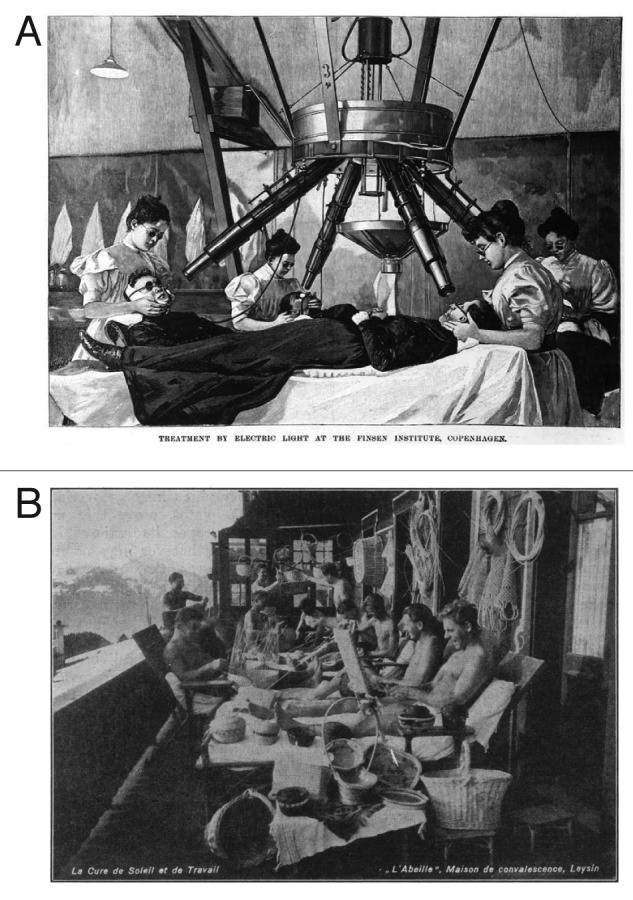
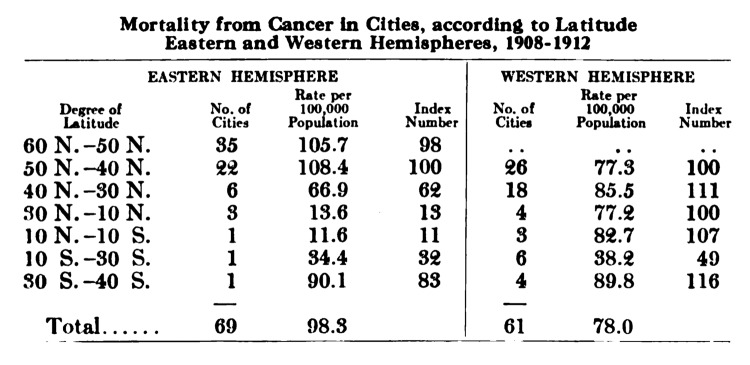
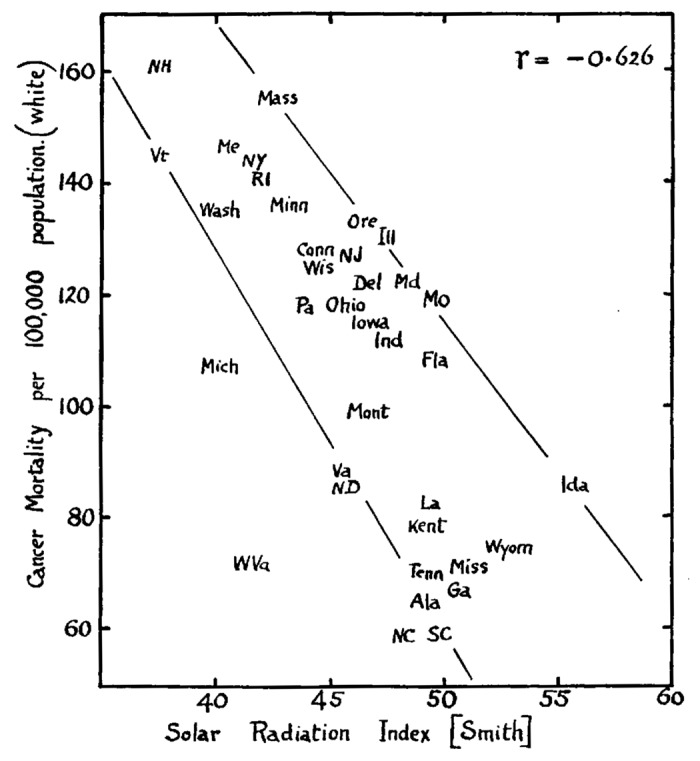
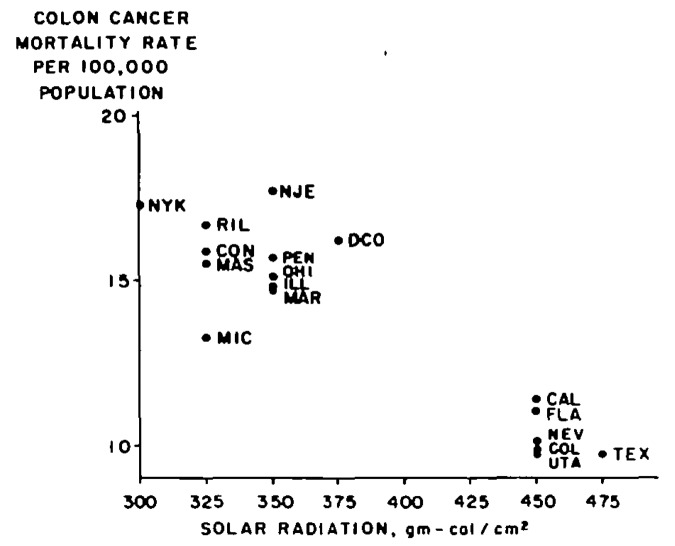
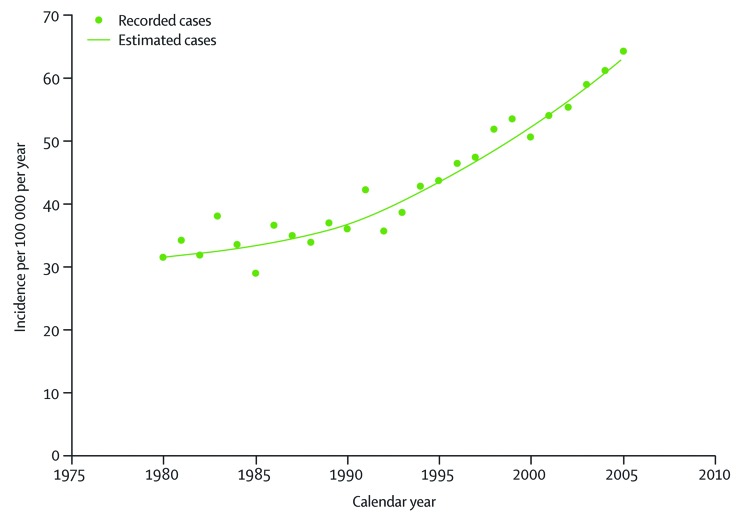
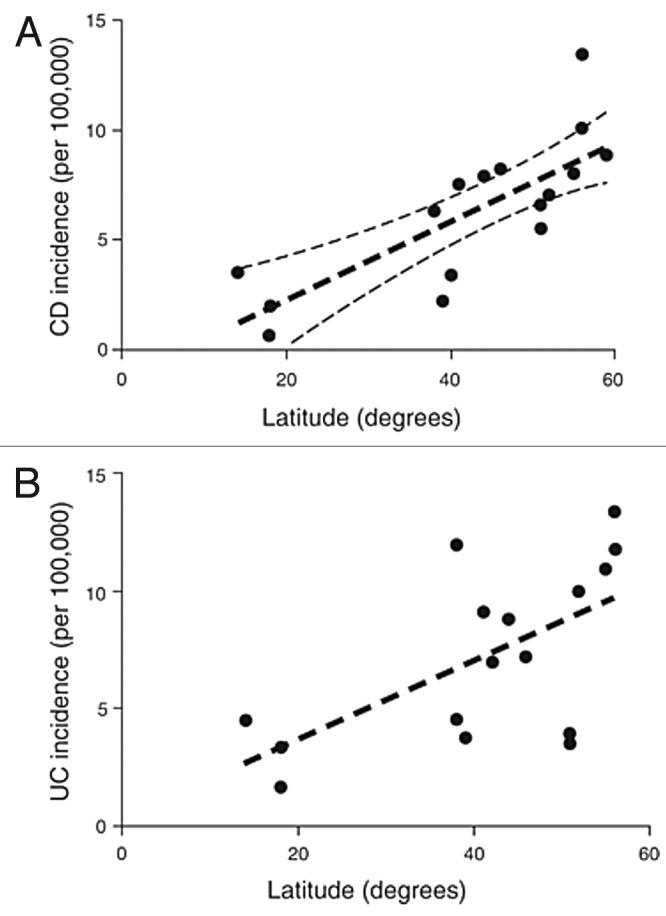
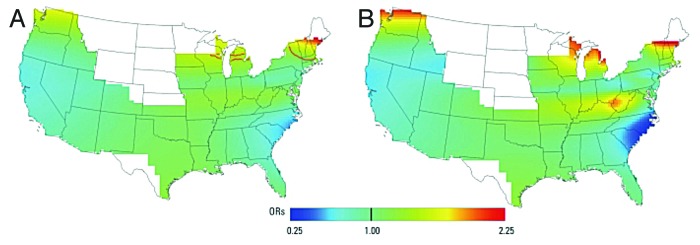
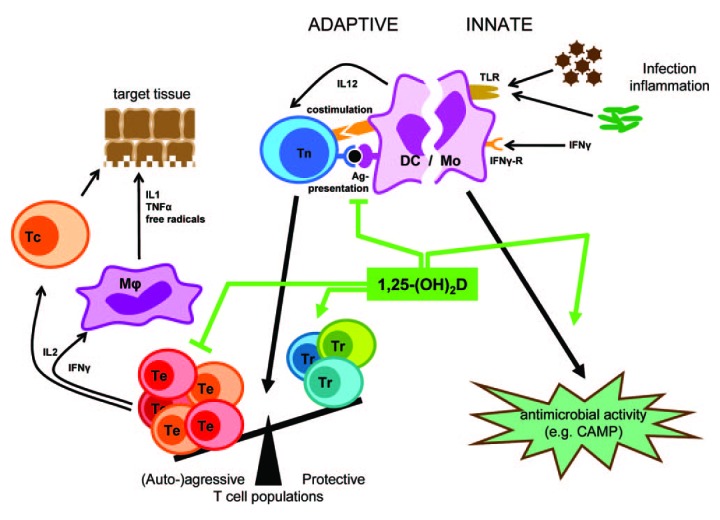
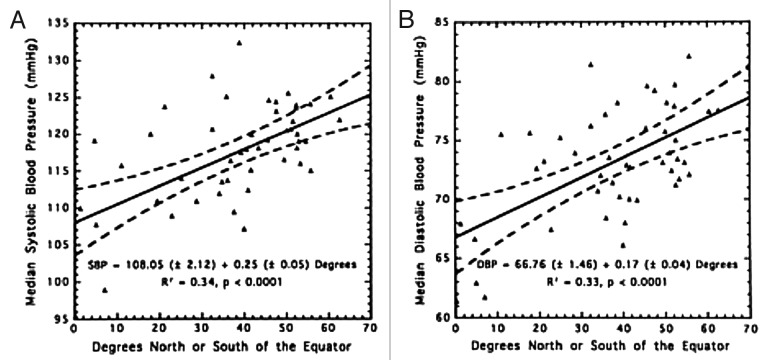
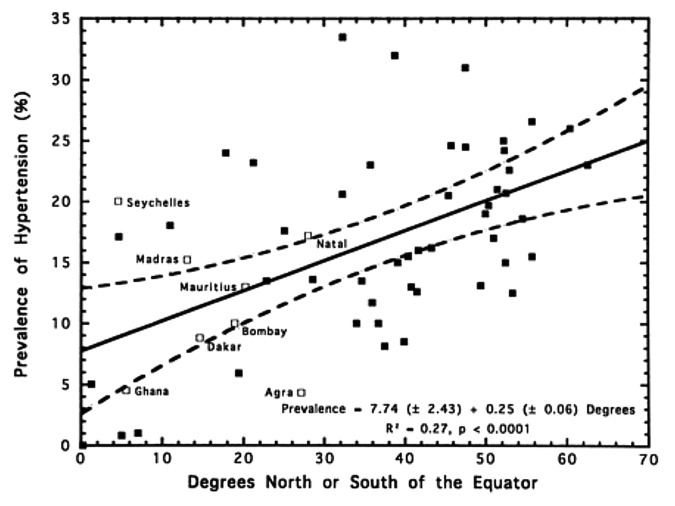
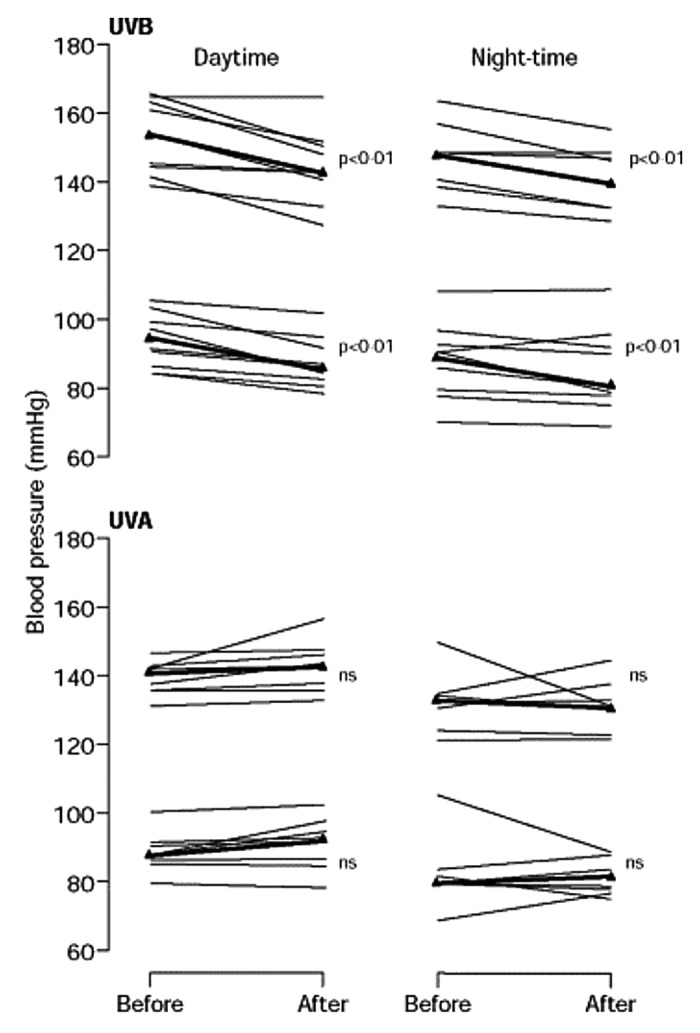
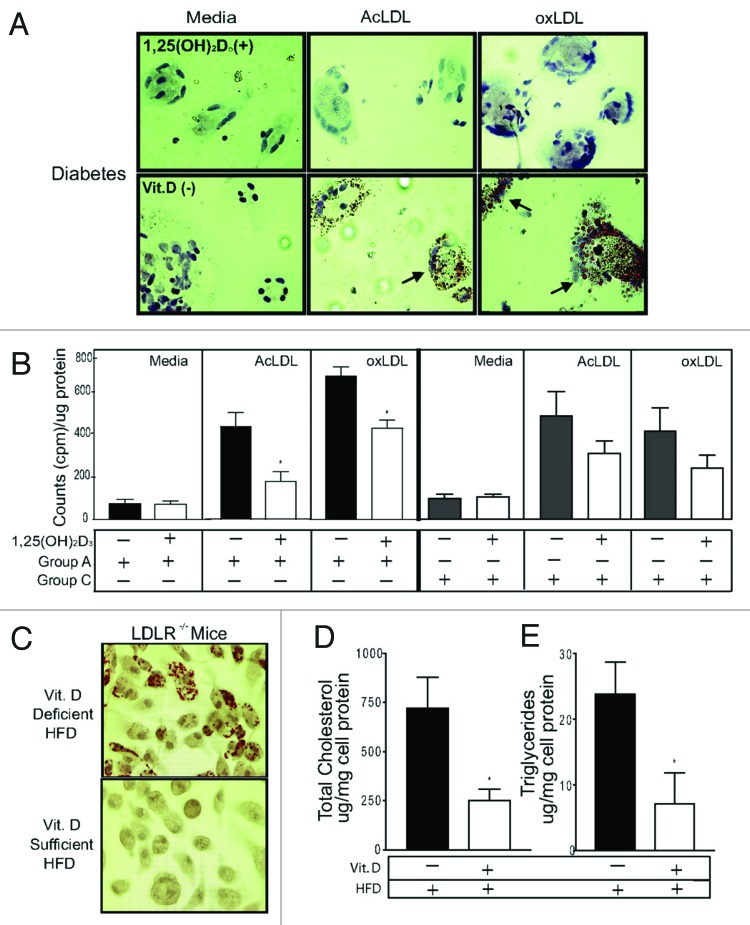
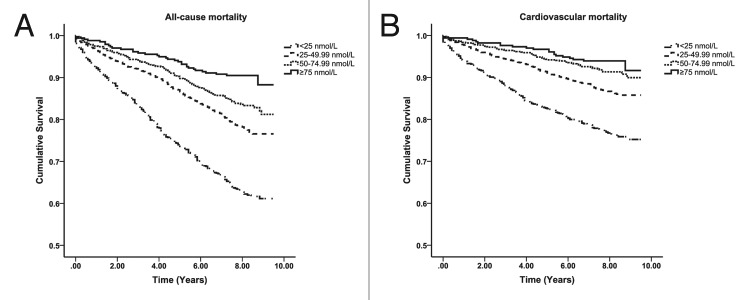
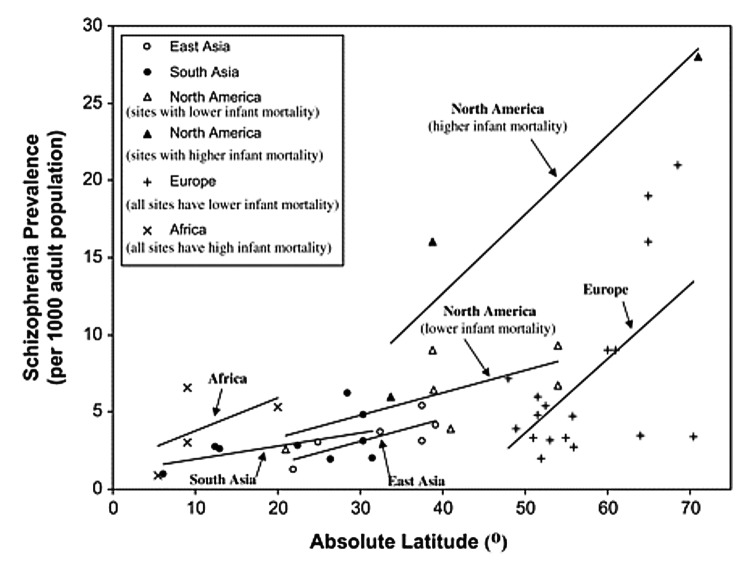
Vitamin D is the sunshine vitamin that has been produced on this earth for more than 500 million years. During exposure to sunlight 7-dehydrocholesterol in the skin absorbs UV B radiation and is converted to previtamin D3 which in turn isomerizes into vitamin D3. Previtamin D3 and vitamin D3 also absorb UV B radiation and are converted into a variety of photoproducts some of which have unique biologic properties. Sun induced vitamin D synthesis is greatly influenced by season, time of day, latitude, altitude, air pollution, skin pigmentation, sunscreen use, passing through glass and plastic, and aging. Vitamin D is metabolized sequentially in the liver and kidneys into 25-hydroxyvitamin D which is a major circulating form and 1,25-dihydroxyvitamin D which is the biologically active form respectively. 1,25-dihydroxyvitamin D plays an important role in regulating calcium and phosphate metabolism for maintenance of metabolic functions and for skeletal health. Most cells and organs in the body have a vitamin D receptor and many cells and organs are able to produce 1,25-dihydroxyvitamin D. As a result 1,25-dihydroxyvitamin D influences a large number of biologic pathways which may help explain association studies relating vitamin D deficiency and living at higher latitudes with increased risk for many chronic diseases including autoimmune diseases, some cancers, cardiovascular disease, infectious disease, schizophrenia and type 2 diabetes. A three-part strategy of increasing food fortification programs with vitamin D, sensible sun exposure recommendations and encouraging ingestion of a vitamin D supplement when needed should be implemented to prevent global vitamin D deficiency and its negative health consequences.
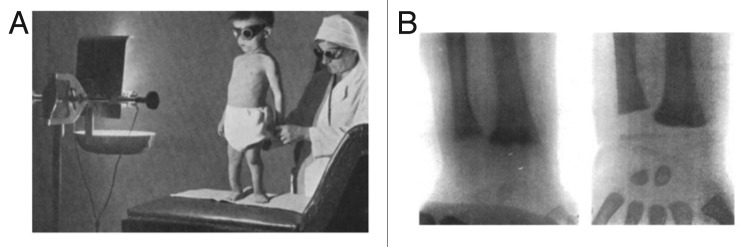
Keywords: 25-hydroxyvitamin D; UV lamp; UV radiation; UVB; autoimmune; cancer; latitude; rickets; sunlight; vitamin D.
Figures














References
-
- Holick M. Phylogenetic and evolutionary aspects of vitamin D from phytoplankton to humans. In: PKT Pang and MP Schreibman (eds), Verebrate Endocrinology: Fundamentals and Biomedical Implications Academic Press, Inc (Harcourt Brace Jovanovich) Orlando, FL 1989;3:7-43.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical