

A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis
- PMID: 24494059
- PMCID: PMC3897595
- DOI: 10.4161/derm.24808
A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis
Abstract
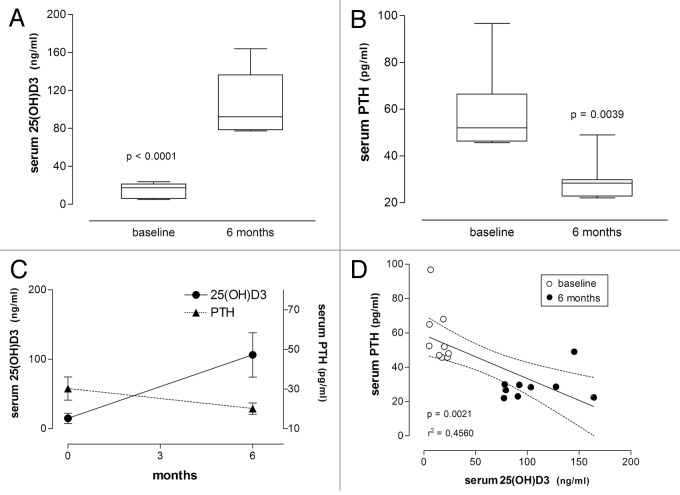
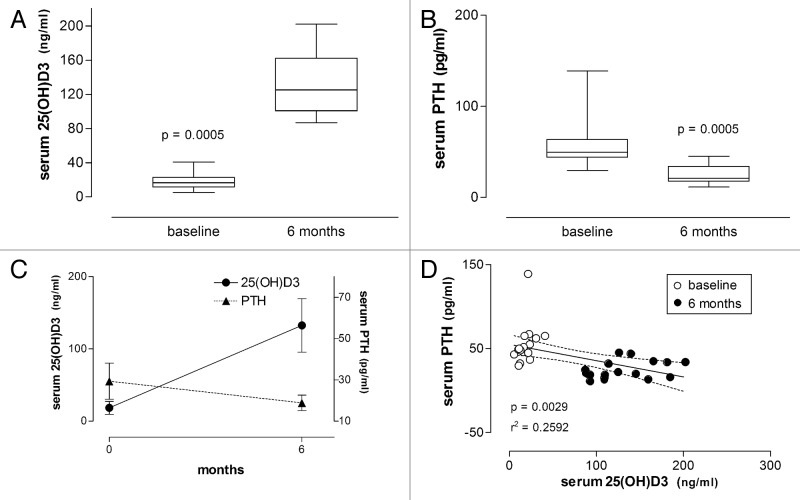
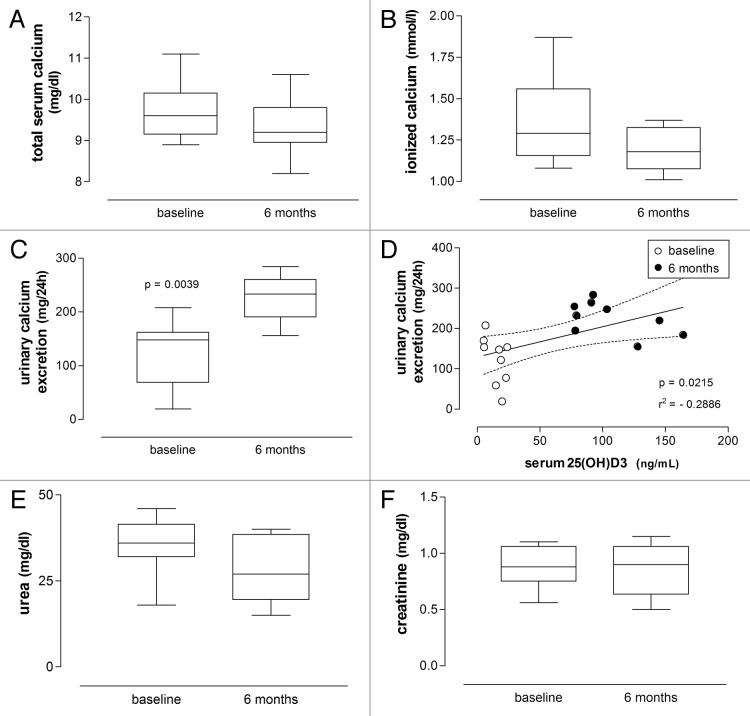
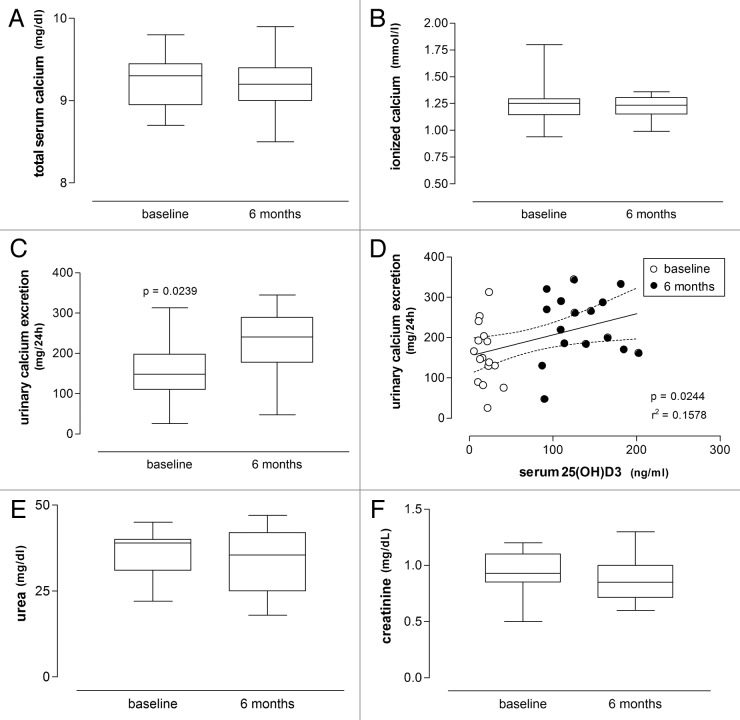
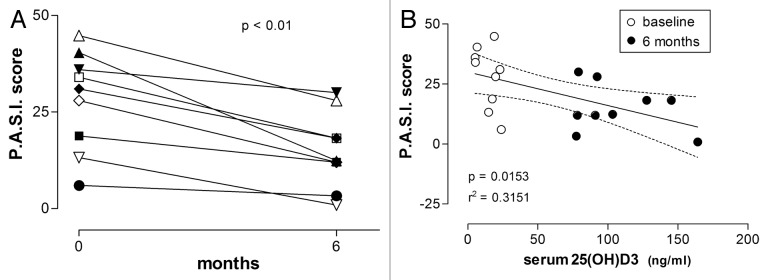
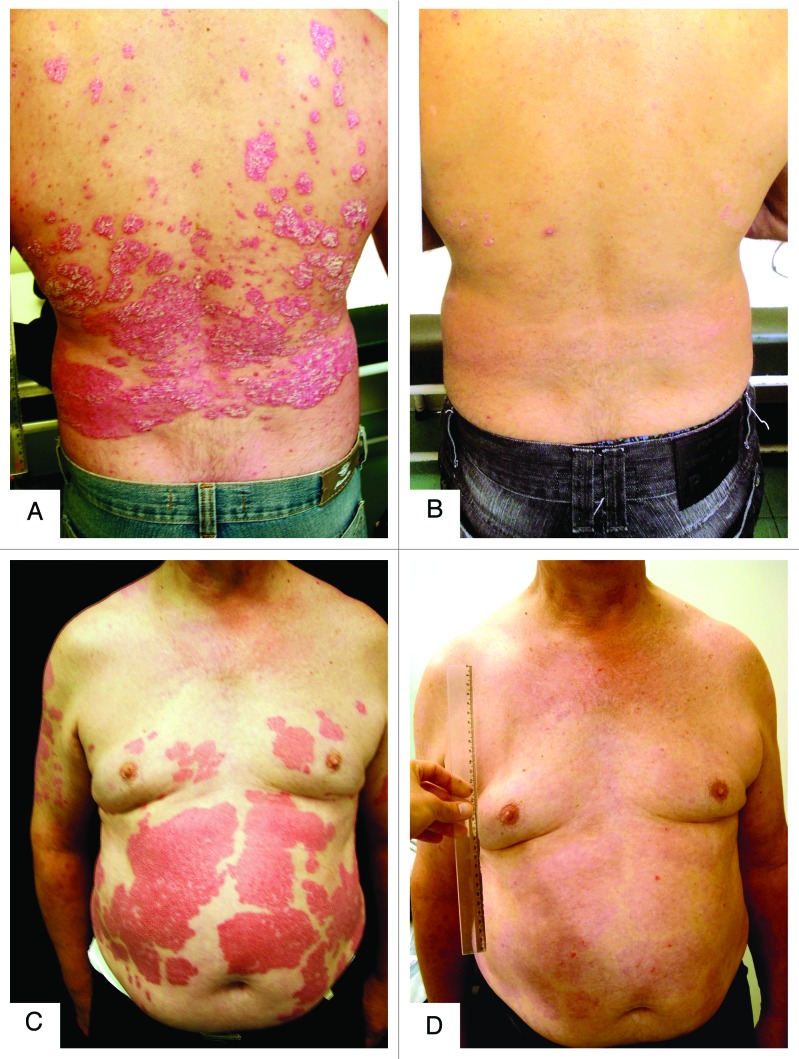
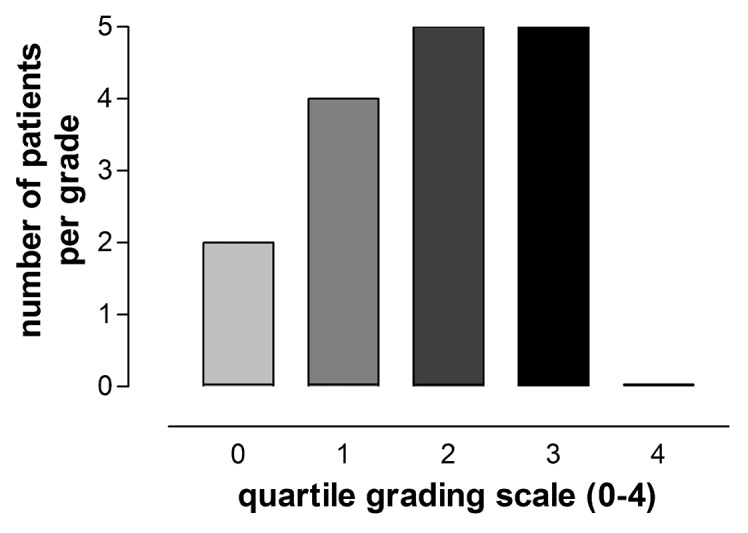
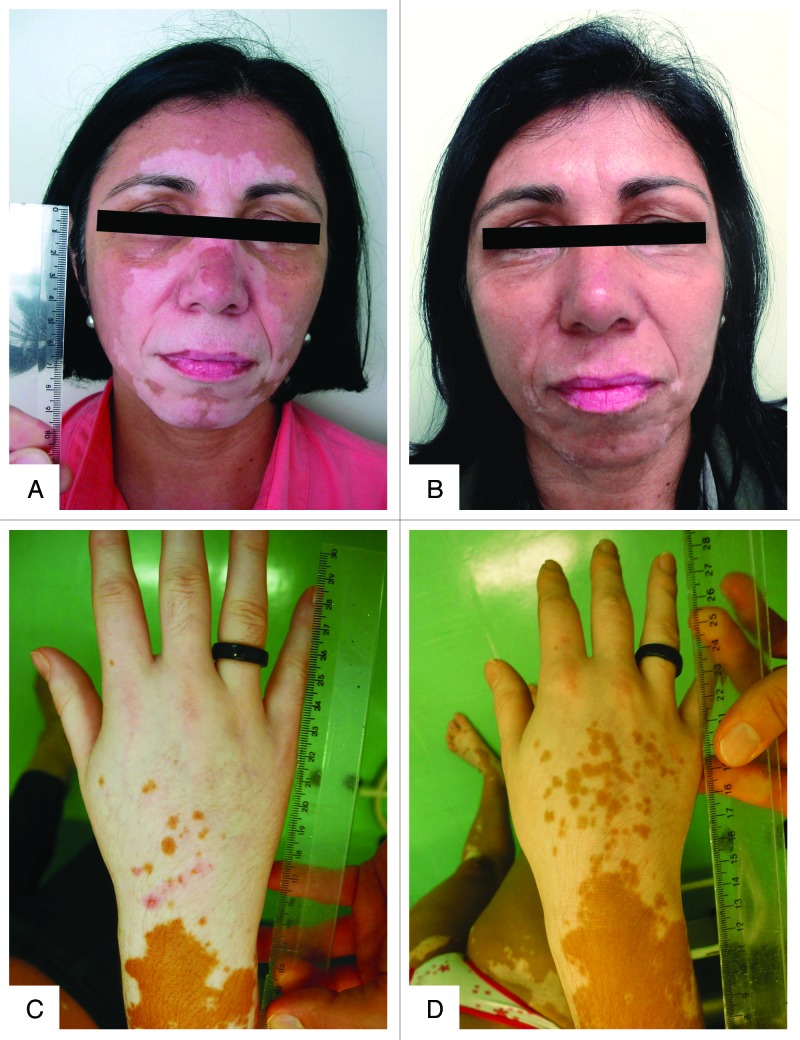
Autoimmunity has been associated with vitamin D deficiency and resistance, with gene polymorphisms related to vitamin D metabolism frequently described in affected patients. High doses of vitamin D3 may conceivably compensate for inherited resistance to its biological effects. This study aimed to assess the efficacy and safety of prolonged high-dose vitamin D3 treatment of patients with psoriasis and vitiligo. Nine patients with psoriasis and 16 patients with vitiligo received vitamin D3 35,000 IU once daily for six months in association with a low-calcium diet (avoiding dairy products and calcium-enriched foods like oat, rice or soya "milk") and hydration (minimum 2.5 L daily). All psoriasis patients were scored according to "Psoriasis Area and Severity Index" (PASI) at baseline and after treatment. Evaluation of clinical response of vitiligo patients required a quartile grading scale. All patients presented low vitamin D status (serum 25(OH)D3 ≤ 30 ng/mL) at baseline. After treatment 25(OH)D3 levels significantly increased (from 14.9 ± 7.4 to 106.3 ± 31.9 ng/mL and from 18.4 ± 8.9 to 132.5 ± 37.0 ng/mL) and PTH levels significantly decreased (from 57.8 ± 16.7 to 28.9 ± 8.2 pg/mL and from 55.3 ± 25.0 to 25.4 ± 10.7 pg/mL) in patients with psoriasis and vitiligo respectively. PTH and 25(OH)D3 serum concentrations correlated inversely. The PASI score significantly improved in all nine patients with psoriasis. Fourteen of 16 patients with vitiligo had 25-75% repigmentation. Serum urea, creatinine and calcium (total and ionized) did not change and urinary calcium excretion increased within the normal range. High-dose vitamin D3 therapy may be effective and safe for vitiligo and psoriasis patients.
Keywords: 25(OH)D3; autoimmunity; calcium; high dose; psoriasis; toxicity; treatment; vitamin D; vitiligo.
Figures
Similar articles
-
[Changes in mineral metabolism in stage 3, 4, and 5 chronic kidney disease (not on dialysis)].Nefrologia. 2008;28 Suppl 3:67-78. Nefrologia. 2008. PMID: 19018742 Spanish.
-
1alpha(OH)D3 One-alpha-hydroxy-cholecalciferol--an active vitamin D analog. Clinical studies on prophylaxis and treatment of secondary hyperparathyroidism in uremic patients on chronic dialysis.Dan Med Bull. 2008 Nov;55(4):186-210. Dan Med Bull. 2008. PMID: 19232159 Review.
-
Prospective Investigation of 25(OH)D3 Serum Concentration Following UVB Narrow Band Phototherapy in Patients with Psoriasis and Atopic Dermatitis.Anticancer Res. 2016 Mar;36(3):1439-44. Anticancer Res. 2016. PMID: 26977048
-
Efficacy of narrowband ultraviolet B phototherapy and levels of serum vitamin D3 in psoriasis: A prospective study.Indian Dermatol Online J. 2016 Mar-Apr;7(2):87-92. doi: 10.4103/2229-5178.178081. Indian Dermatol Online J. 2016. PMID: 27057487 Free PMC article.
-
1-alpha-Hydroxyvitamin D3 derivatives in the treatment of renal bone diseases: justification and optimal modalities of administration.Nephron. 1995;71(3):254-83. doi: 10.1159/000188732. Nephron. 1995. PMID: 8569975 Review.
Cited by
-
Nongenomic Activities of Vitamin D.Nutrients. 2022 Dec 1;14(23):5104. doi: 10.3390/nu14235104. Nutrients. 2022. PMID: 36501134 Free PMC article. Review.
-
Dietary Interventions, Supplements, and Plant-Derived Compounds for Adjunct Vitiligo Management: A Review of the Literature.Nutrients. 2025 Jan 20;17(2):357. doi: 10.3390/nu17020357. Nutrients. 2025. PMID: 39861486 Free PMC article. Review.
-
Vitamin D and Its Potential Benefit for the COVID-19 Pandemic.Endocr Pract. 2021 May;27(5):484-493. doi: 10.1016/j.eprac.2021.03.006. Epub 2021 Mar 17. Endocr Pract. 2021. PMID: 33744444 Free PMC article. Review.
-
Oral Vitamin D Therapy in Patients with Psoriasis.Nutrients. 2021 Jan 6;13(1):163. doi: 10.3390/nu13010163. Nutrients. 2021. PMID: 33419149 Free PMC article. Review.
-
Skin Disorders and Osteoporosis: Unraveling the Interplay Between Vitamin D, Microbiota, and Epigenetics Within the Skin-Bone Axis.Int J Mol Sci. 2024 Dec 28;26(1):179. doi: 10.3390/ijms26010179. Int J Mol Sci. 2024. PMID: 39796035 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources