

Subaxial cervical spine trauma: evaluation and surgical decision-making
- PMID: 24494184
- PMCID: PMC3908983
- DOI: 10.1055/s-0033-1356764
Subaxial cervical spine trauma: evaluation and surgical decision-making
Abstract
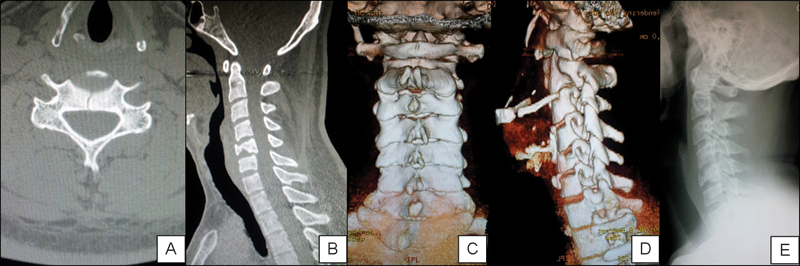
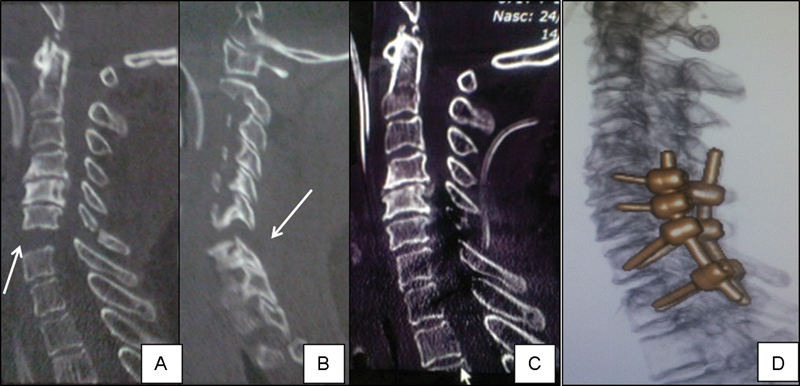
Study Design Literature review. Objective To discuss the evaluation and management of subaxial cervical spine trauma (C3-7). Methods A literature review of the main imaging modalities, classification systems, and nonsurgical and surgical treatment performed. Results Computed tomography and reconstructions allow for accurate radiologic identification of subaxial cervical spine trauma in most cases. Magnetic resonance imaging can be utilized to evaluate the stabilizing discoligamentous complex, the nerves, and the spinal cord. The Subaxial Injury Classification (SLIC) is a new system that aids in injury classification and helps guide the decision-making process of conservative versus surgical treatment. Though promising, the SLIC system requires further validation. When the decision for surgical treatment is made, early decompression (less than 24 hours) has been associated with better neurologic recovery. Surgical treatment should be individualized based on the injury characteristics and surgeon's preferences. Conclusions The current state of subaxial cervical spine trauma is one of great progress. However, many questions remain unanswered. We need to continue to account for the individual patient, surgeon, and hospital circumstances that effect decision making and care.
Keywords: classification; diagnosis; subaxial cervical spine trauma; treatment.
Conflict of interest statement
Figures
References
-
- Joaquim A F, Patel A P. Occipito-cervical trauma: evaluation, classification and treatment. Contemporary Spine Surgery. 2010;11(4):1–5.
-
- Joaquim A F, Patel A P. Occipito-cervical trauma: evaluation, classification and treatment. Contemporary Neurosurgery. 2010;32(12):1–6.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
