

Impact of methodology on estrogens' effects on cerebral ischemia in rats: an updated meta-analysis
- PMID: 24495535
- PMCID: PMC3975994
- DOI: 10.1186/1471-2202-15-22
Impact of methodology on estrogens' effects on cerebral ischemia in rats: an updated meta-analysis
Abstract
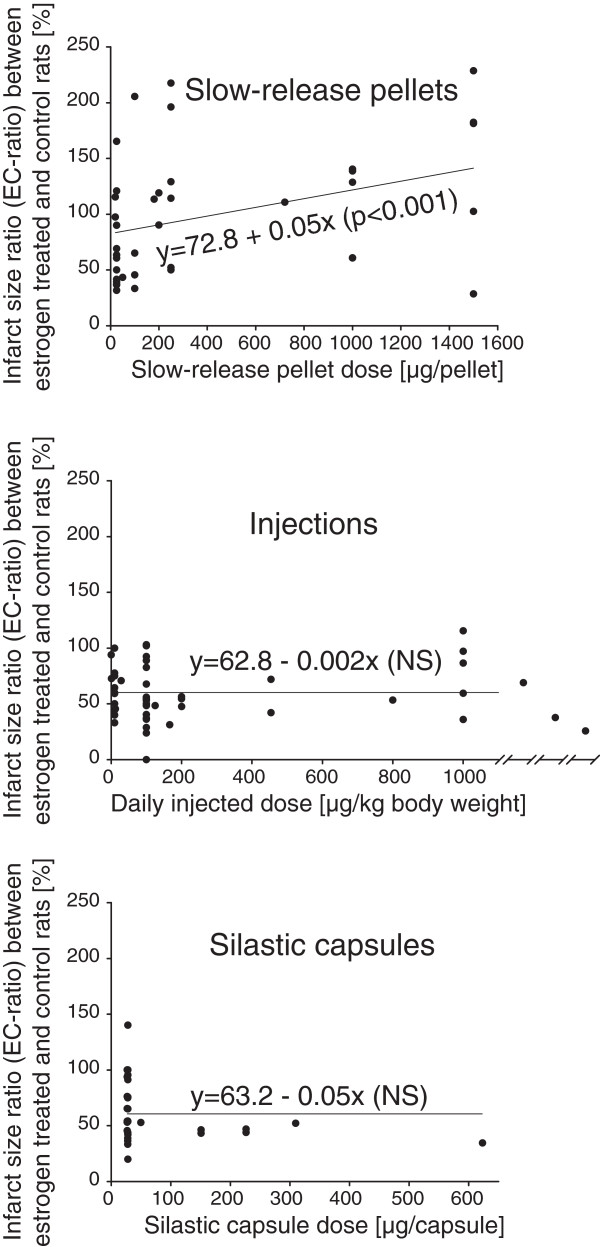
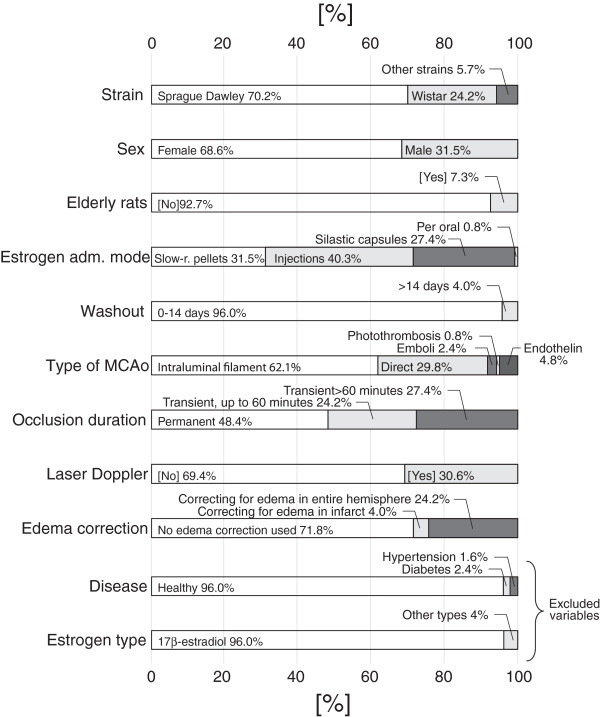
Background: Although most animal stroke studies have demonstrated potent neuroprotective effects of estrogens, there are a number of articles reporting the opposite. In 2009, we made the case that this dichotomy was related to administered estrogen dose. Several other suggestions for the discordant results have also been propagated, including the age of the experimental animals and the length of hypoestrogenicity prior to estrogen administration. These two suggestions have gained much popularity, probably because of their kinship with the window of opportunity hypothesis, which is commonly used to explain the analogous dichotomy among human studies. We were therefore encouraged to perform an updated meta-analysis, and to improve it by including all relevant variables in a large multiple regression model, where the impact of confounders could be controlled for.
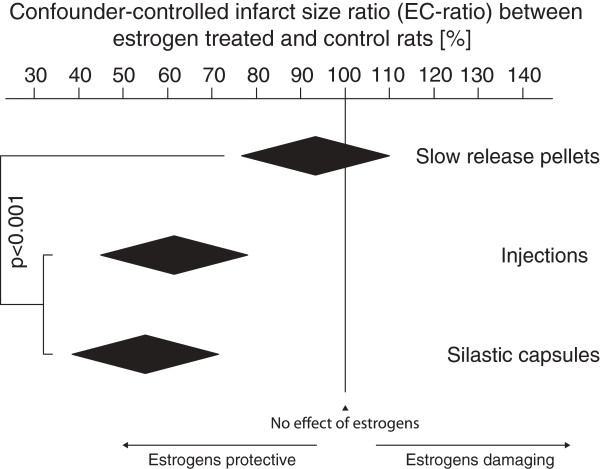
Results: The multiple regression model revealed an indisputable impact of estrogen administration mode on the effects of estrogens in ischemic stroke. Subcutaneous slow-release pellets differed from the injection and silastic capsule treatments in terms of impact of estrogens on ischemic stroke, showing that the first mentioned were more prone to render estrogens damaging. Neither the use of elderly animals nor the adoption of longer wash-out periods influenced estrogens' effects on experimental ischemic stroke in rats.
Conclusions: We conclude that the discordant results regarding estrogens' effects in rat models of ischemic stroke are a consequence of differences in estrogen administration modes. These results are not only of importance for the ongoing debate regarding menopausal hormone therapy, but also have an important bearing on experimental stroke methodology and the apparent translational roadblock for suggested stroke interventions.
Figures
References
-
- Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, Jackson RD, Beresford SA, Howard BV, Johnson KC. et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA. 2002;15(3):321–333. doi: 10.1001/jama.288.3.321. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
