

Performance of four computer-coded verbal autopsy methods for cause of death assignment compared with physician coding on 24,000 deaths in low- and middle-income countries
- PMID: 24495855
- PMCID: PMC3912488
- DOI: 10.1186/1741-7015-12-20
Performance of four computer-coded verbal autopsy methods for cause of death assignment compared with physician coding on 24,000 deaths in low- and middle-income countries
Abstract
Background: Physician-coded verbal autopsy (PCVA) is the most widely used method to determine causes of death (CODs) in countries where medical certification of death is uncommon. Computer-coded verbal autopsy (CCVA) methods have been proposed as a faster and cheaper alternative to PCVA, though they have not been widely compared to PCVA or to each other.
Methods: We compared the performance of open-source random forest, open-source tariff method, InterVA-4, and the King-Lu method to PCVA on five datasets comprising over 24,000 verbal autopsies from low- and middle-income countries. Metrics to assess performance were positive predictive value and partial chance-corrected concordance at the individual level, and cause-specific mortality fraction accuracy and cause-specific mortality fraction error at the population level.
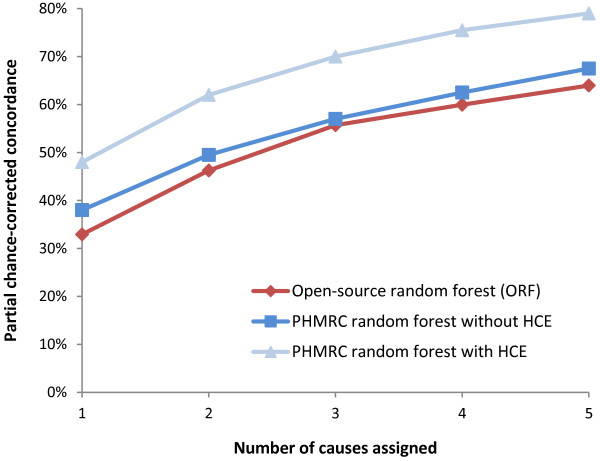
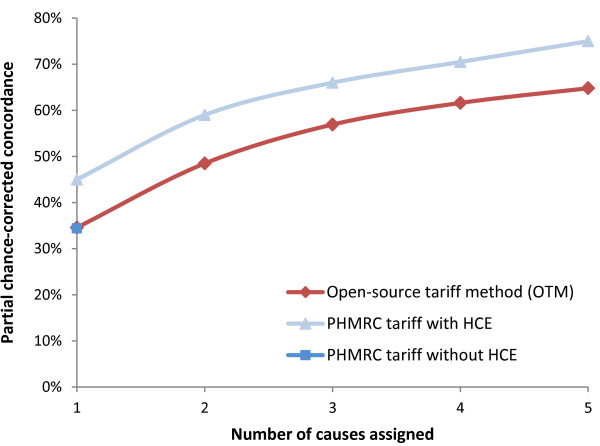
Results: The positive predictive value for the most probable COD predicted by the four CCVA methods averaged about 43% to 44% across the datasets. The average positive predictive value improved for the top three most probable CODs, with greater improvements for open-source random forest (69%) and open-source tariff method (68%) than for InterVA-4 (62%). The average partial chance-corrected concordance for the most probable COD predicted by the open-source random forest, open-source tariff method and InterVA-4 were 41%, 40% and 41%, respectively, with better results for the top three most probable CODs. Performance generally improved with larger datasets. At the population level, the King-Lu method had the highest average cause-specific mortality fraction accuracy across all five datasets (91%), followed by InterVA-4 (72% across three datasets), open-source random forest (71%) and open-source tariff method (54%).
Conclusions: On an individual level, no single method was able to replicate the physician assignment of COD more than about half the time. At the population level, the King-Lu method was the best method to estimate cause-specific mortality fractions, though it does not assign individual CODs. Future testing should focus on combining different computer-coded verbal autopsy tools, paired with PCVA strengths. This includes using open-source tools applied to larger and varied datasets (especially those including a random sample of deaths drawn from the population), so as to establish the performance for age- and sex-specific CODs.
Figures
Similar articles
-
Comparison of physician-certified verbal autopsy with computer-coded verbal autopsy for cause of death assignment in hospitalized patients in low- and middle-income countries: systematic review.BMC Med. 2014 Feb 4;12:22. doi: 10.1186/1741-7015-12-22. BMC Med. 2014. PMID: 24495312 Free PMC article.
-
Using verbal autopsy to measure causes of death: the comparative performance of existing methods.BMC Med. 2014 Jan 9;12:5. doi: 10.1186/1741-7015-12-5. BMC Med. 2014. PMID: 24405531 Free PMC article.
-
Agreement between cause of death assignment by computer-coded verbal autopsy methods and physician coding of verbal autopsy interviews in South Africa.Glob Health Action. 2023 Dec 31;16(1):2285105. doi: 10.1080/16549716.2023.2285105. Epub 2023 Dec 1. Glob Health Action. 2023. PMID: 38038664 Free PMC article.
-
Evaluation of methods for assigning causes of death from verbal autopsies in India.Front Big Data. 2023 Aug 24;6:1197471. doi: 10.3389/fdata.2023.1197471. eCollection 2023. Front Big Data. 2023. PMID: 37693847 Free PMC article.
-
Verbal autopsy models in determining causes of death.Trop Med Int Health. 2021 Dec;26(12):1560-1567. doi: 10.1111/tmi.13678. Epub 2021 Sep 30. Trop Med Int Health. 2021. PMID: 34498340
Cited by
-
Nationwide evaluation of malaria infections, morbidity, mortality, and coverage of malaria control interventions in Madagascar.Malar J. 2014 Nov 28;13:465. doi: 10.1186/1475-2875-13-465. Malar J. 2014. PMID: 25431003 Free PMC article.
-
Naive Bayes classifiers for verbal autopsies: comparison to physician-based classification for 21,000 child and adult deaths.BMC Med. 2015 Nov 25;13:286. doi: 10.1186/s12916-015-0521-2. BMC Med. 2015. PMID: 26607695 Free PMC article.
-
Local perceptions of causes of death in rural South Africa: a comparison of perceived and verbal autopsy causes of death.Glob Health Action. 2015 Jul 17;8:28302. doi: 10.3402/gha.v8.28302. eCollection 2015. Glob Health Action. 2015. PMID: 26193897 Free PMC article.
-
What are our options for mortality data collection and how can they provide HIV-specific information?J Public Health Afr. 2025 May 27;16(1):733. doi: 10.4102/jphia.v16i1.733. eCollection 2025. J Public Health Afr. 2025. PMID: 40469402 Free PMC article. Review.
-
Comparing verbal autopsy cause of death findings as determined by physician coding and probabilistic modelling: a public health analysis of 54 000 deaths in Africa and Asia.J Glob Health. 2015 Jun;5(1):010402. doi: 10.7189/jogh.05.010402. J Glob Health. 2015. PMID: 25734004 Free PMC article.
References
-
- Jha P. Counting the dead is one of the world’s best investments to reduce premature mortality. Hypothesis. 2012;10:e3.
-
- Health and Demographic Surveillance Unit. Health and Demographic Surveillance System: Matlab. Volume 36: Registration of Health and Demographic Events 2003. Dhaka: ICDDR, B; 2005.
-
- King G, Lu Y. Verbal autopsy methods with multiple causes of death. Statistical Science. 2008;23:78–91. doi: 10.1214/07-STS247. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
