

Cerebral neovascularization in diabetes: implications for stroke recovery and beyond
- PMID: 24496174
- PMCID: PMC3982092
- DOI: 10.1038/jcbfm.2014.18
Cerebral neovascularization in diabetes: implications for stroke recovery and beyond
Abstract
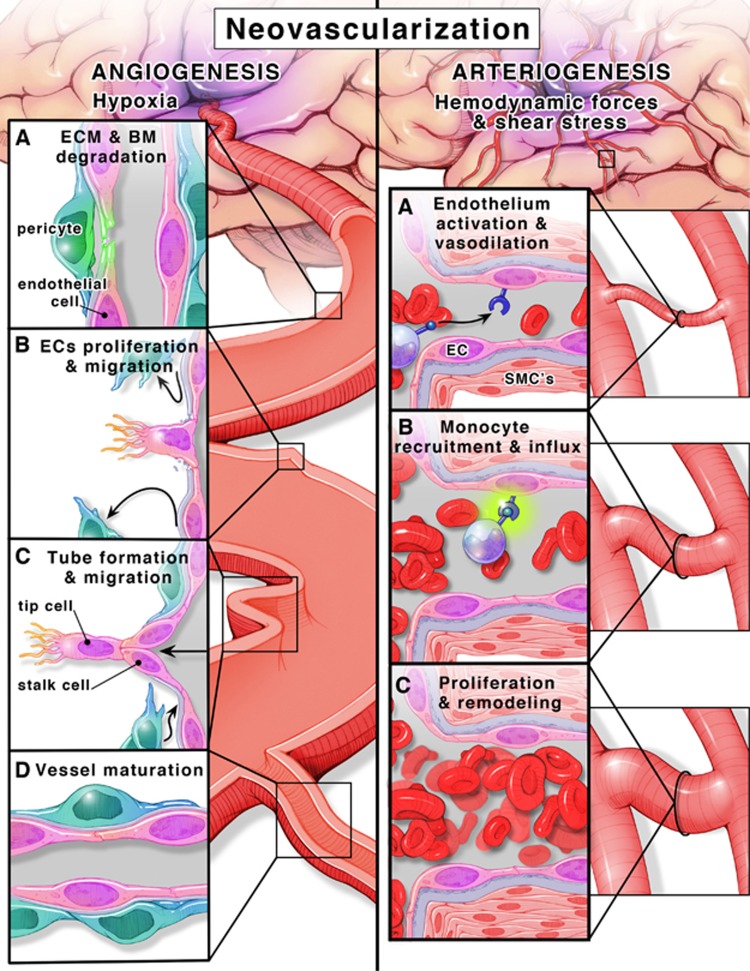
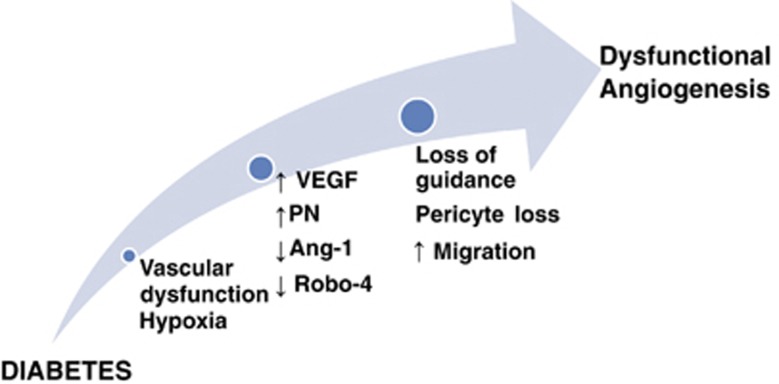
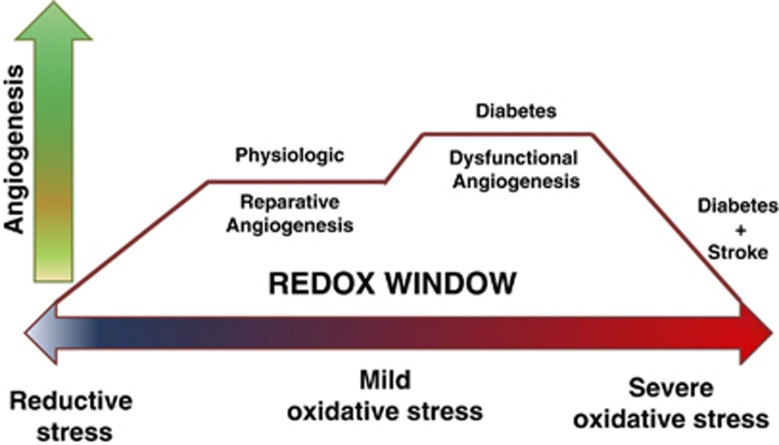
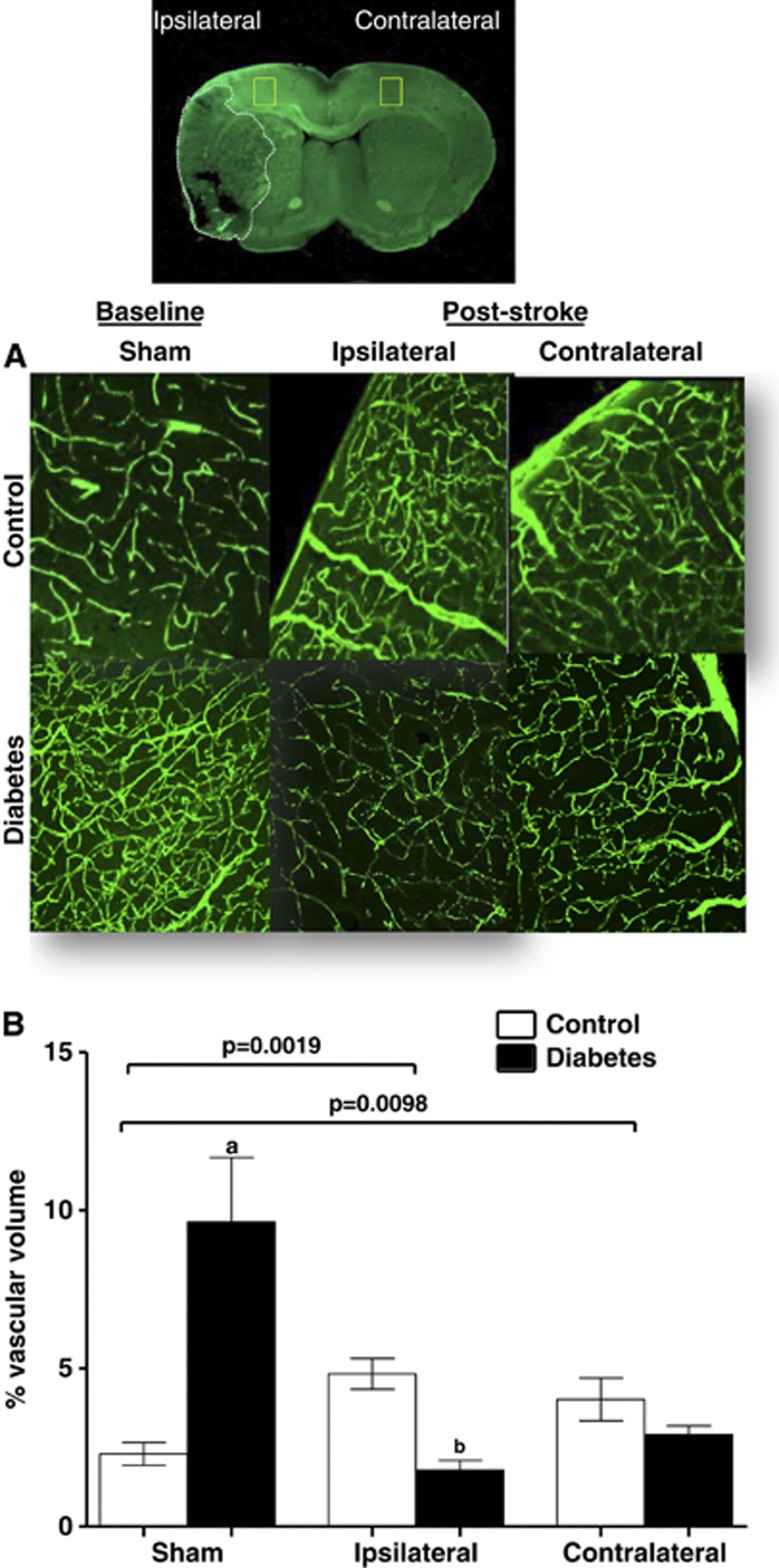
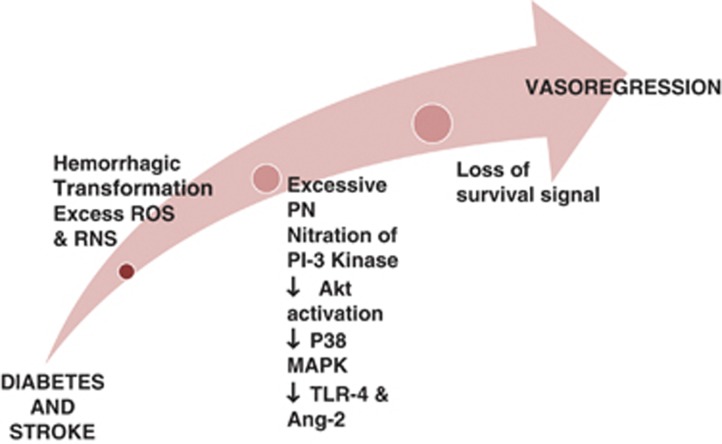
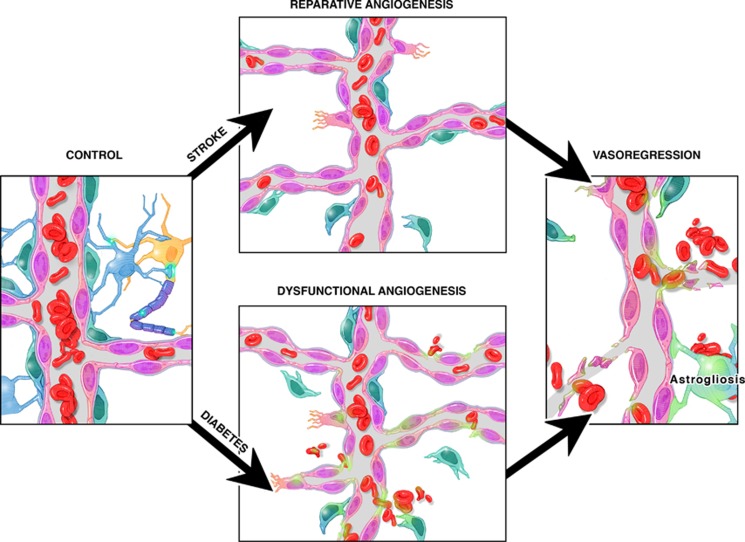
Neovascularization is an innate physiologic response by which tissues respond to various stimuli through collateral remodeling (arteriogenesis) and new vessel formation from existing vessels (angiogenesis) or from endothelial progenitor cells (vasculogenesis). Diabetes has a major impact on the neovascularization process but the response varies between different organ systems. While excessive angiogenesis complicates diabetic retinopathy, impaired neovascularization contributes to coronary and peripheral complications of diabetes. How diabetes influences cerebral neovascularization remained unresolved until recently. Diabetes is also a major risk factor for stroke and poor recovery after stroke. In this review, we discuss the impact of diabetes, stroke, and diabetic stroke on cerebral neovascularization, explore potential mechanisms involved in diabetes-mediated neovascularization as well as the effects of the diabetic milieu on poststroke neovascularization and recovery, and finally discuss the clinical implications of these effects.
Figures
References
-
- Mink JW, Blumenschine RJ, Adams DB. Ratio of central nervous system to body metabolism in vertebrates: its constancy and functional basis. Am J Physiol. 1981;241:R203–R212. - PubMed
-
- Quaegebeur A, Lange C, Carmeliet P. The neurovascular link in health and disease: molecular mechanisms and therapeutic implications. Neuron. 2011;71:406–424. - PubMed
-
- Begley DJ, Brightman MW. Structural and functional aspects of the blood-brain barrier. Prog Drug Res. 2003;61:39–78. - PubMed
-
- Cipolla MJ.The cerebral circulationIn: Granger NGaJ, (ed). Integrated systems physiology: from molecule to function Morgan & Claypool Life Sciences: San Rafael (CA)2009 - PubMed
-
- Xu K, Lamanna JC. Chronic hypoxia and the cerebral circulation. J Appl Physiol. 2006;100:725–730. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
