

Patterns of statin initiation, intensification, and maximization among patients hospitalized with an acute myocardial infarction
- PMID: 24496318
- PMCID: PMC4103689
- DOI: 10.1161/CIRCULATIONAHA.113.003589
Patterns of statin initiation, intensification, and maximization among patients hospitalized with an acute myocardial infarction
Abstract
Background: Intensive statins are superior to moderate statins in reducing morbidity and mortality after an acute myocardial infarction. Although studies have documented rates of statin prescription as a quality performance measure, variations in hospitals' rates of initiating, intensifying, and maximizing statin therapy after acute myocardial infarction are unknown.
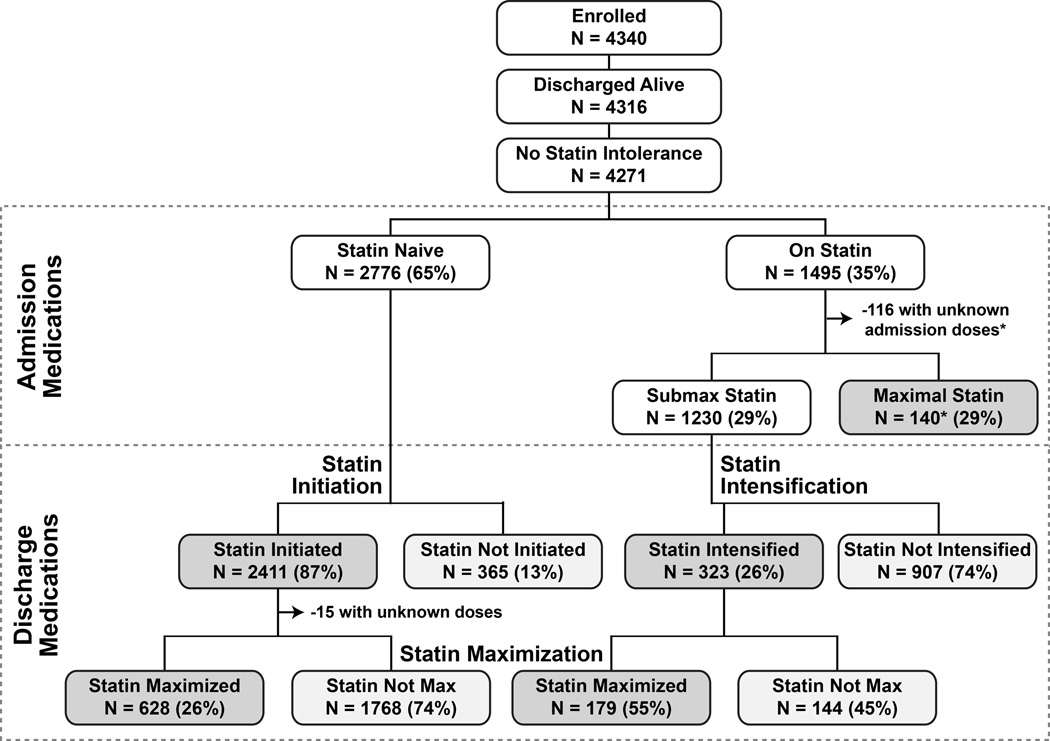
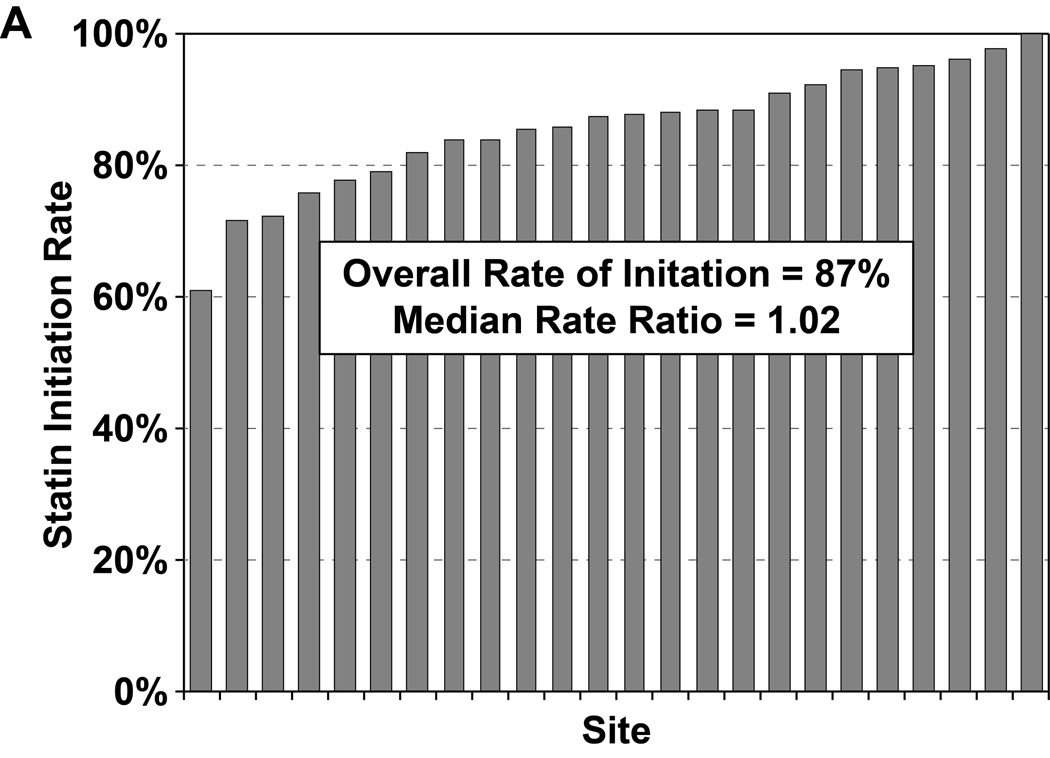
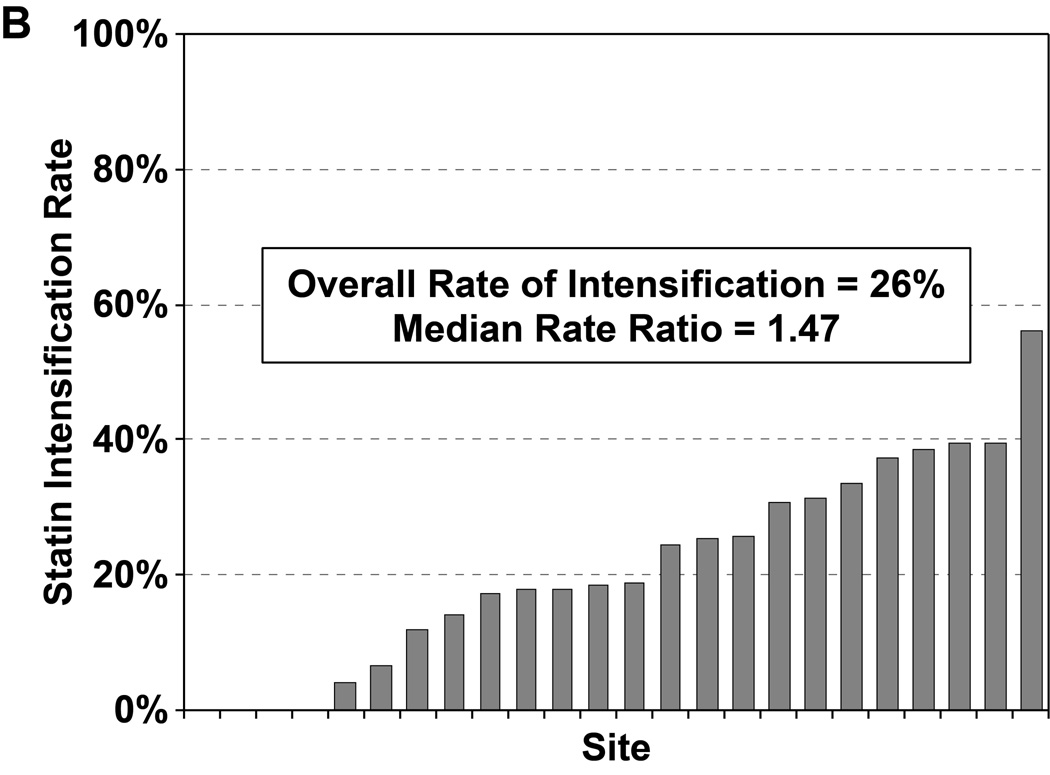
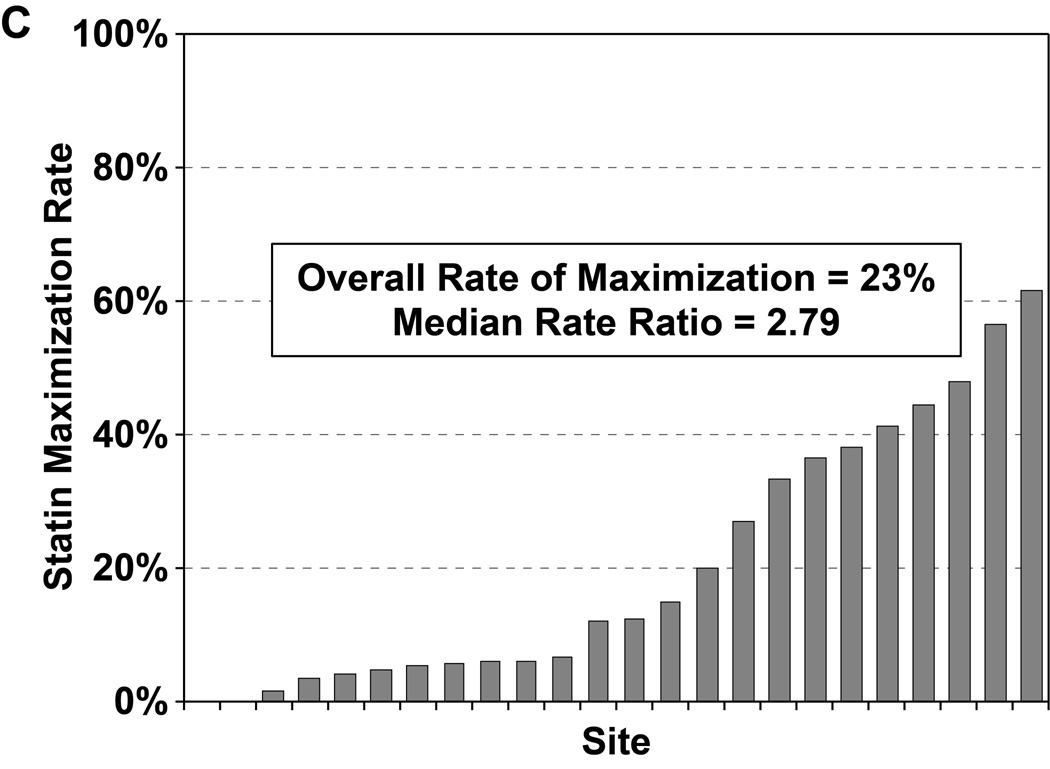
Methods and results: We assessed statin use at admission and discharge among 4340 acute myocardial infarction patients from 24 US hospitals (2005-2008). Hierarchical models estimated site variation in statin initiation in naïve patients, intensification in those undergoing submaximal therapy, and discharge on maximal therapy (defined as a statin with expected low-density lipoprotein cholesterol lowering ≥ 50%) after adjustment for patient factors, including low-density lipoprotein cholesterol level. Site variation was explored with a median rate ratio, which estimates the relative difference in risk ratios of 2 hypothetically identical patients at 2 different hospitals. Among statin-naïve patients, 87% without a contraindication were prescribed a statin, with no variability across sites (median rate ratio, 1.02). Among patients who arrived on submaximal statins, 26% had their statin therapy intensified, with modest site variability (median rate ratio, 1.47). Among all patients without a contraindication, 23% were discharged on maximal statin therapy, with substantial hospital variability (median rate ratio, 2.79).
Conclusions: In a large, multicenter acute myocardial infarction cohort, statin therapy was begun in nearly 90% of patients during hospitalization, with no variability across sites; however, rates of statin intensification and maximization were low and varied substantially across hospitals. Given that more intense statin therapy is associated with better outcomes, changing the existing performance measures to include the intensity of statin therapy may improve care.
Keywords: lipids; myocardial infarction; secondary prevention; statins, HMG-CoA.
Conflict of interest statement
Figures
Comment in
-
The quality of quality: is it time for new tools?Circulation. 2014 Mar 25;129(12):1270-2. doi: 10.1161/CIRCULATIONAHA.114.008390. Epub 2014 Feb 4. Circulation. 2014. PMID: 24496319 Free PMC article. No abstract available.
References
-
- Mrc/bhf heart protection study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial. Lancet. 2002;360:7–22. - PubMed
-
- LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: A meta-analysis of randomized controlled trials. JAMA. 1999;282:2340–2346. - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE, 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC, Jr, Jacobs AK, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B. Acc/aha 2007 guidelines for the management of patients with unstable angina/non st-elevation myocardial infarction: A report of the american college of cardiology/american heart association task force on practice guidelines (writing committee to revise the 2002 guidelines for the management of patients with unstable angina/non st-elevation myocardial infarction): Developed in collaboration with the american college of emergency physicians, the society for cardiovascular angiography and interventions, and the society of thoracic surgeons: Endorsed by the american association of cardiovascular and pulmonary rehabilitation and the society for academic emergency medicine. Circulation. 2007;116:e148–e304. - PubMed
-
- Kushner FG, Hand M, Smith SC, Jr, King SB, 3rd, Anderson JL, Antman EM, Bailey SR, Bates ER, Blankenship JC, Casey DE, Jr, Green LA, Hochman JS, Jacobs AK, Krumholz HM, Morrison DA, Ornato JP, Pearle DL, Peterson ED, Sloan MA, Whitlow PL, Williams DO. 2009 focused updates: Acc/aha guidelines for the management of patients with st-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and acc/aha/scai guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): A report of the american college of cardiology foundation/american heart association task force on practice guidelines. Circulation. 2009;120:2271–2306. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
