

Blood pressure trajectories in early adulthood and subclinical atherosclerosis in middle age
- PMID: 24496536
- PMCID: PMC4122296
- DOI: 10.1001/jama.2013.285122
Blood pressure trajectories in early adulthood and subclinical atherosclerosis in middle age
Erratum in
- JAMA. 2014 Apr 16;311(15):1568
Abstract
Importance: Single measures of blood pressure (BP) levels are associated with the development of atherosclerosis; however, long-term patterns in BP and their effect on cardiovascular disease risk are poorly characterized.
Objectives: To identify common BP trajectories throughout early adulthood and to determine their association with presence of coronary artery calcification (CAC) during middle age.
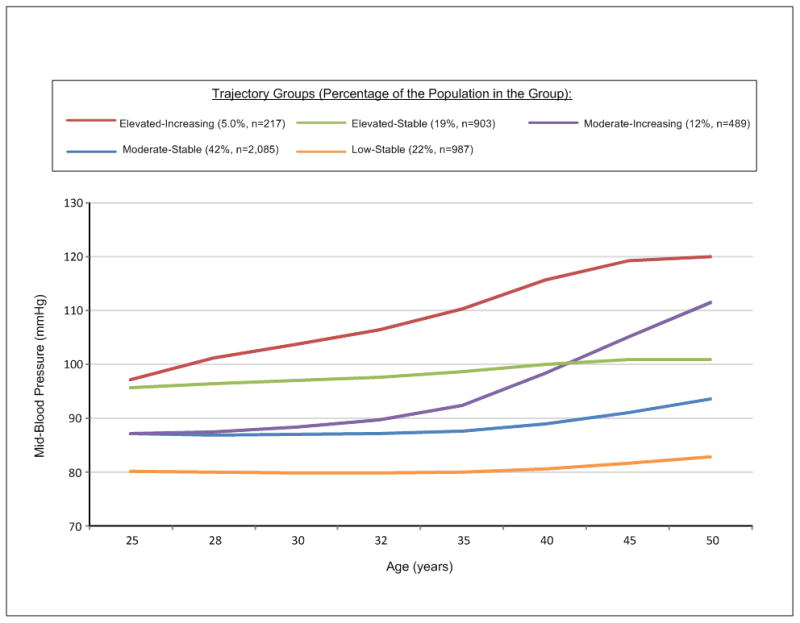
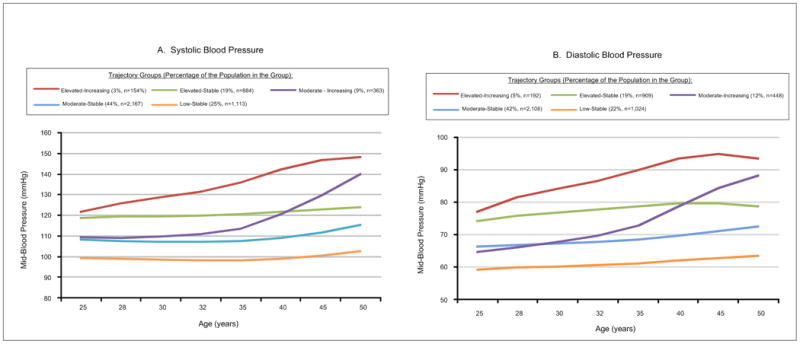
Design, setting, and participants: Prospective cohort data from 4681 participants in the CARDIA study, who were black and white men and women aged 18 to 30 years at baseline in 1985-1986 at 4 urban US sites, collected through 25 years of follow-up (2010-2011). We examined systolic BP, diastolic BP, and mid-BP (calculated as [SBP+DBP]/2, an important marker of coronary heart disease risk among younger populations) at baseline and years 2, 5, 7, 10, 15, 20, and 25. Latent mixture modeling was used to identify trajectories in systolic, diastolic, and mid-BP over time.
Main outcomes and measures: Coronary artery calcification greater than or equal to Agatston score of 100 Hounsfield units (HU) at year 25.
Results: We identified 5 distinct mid-BP trajectories: low-stable (21.8%; 95% CI, 19.9%-23.7%; n=987), moderate-stable (42.3%; 40.3%-44.3%; n=2085), moderate-increasing (12.2%; 10.4%-14.0%; n=489), elevated-stable (19.0%; 17.1%-20.0%; n=903), and elevated-increasing (4.8%; 4.0%-5.5%; n=217). Compared with the low-stable group, trajectories with elevated BP levels had greater odds of having a CAC score of 100 HU or greater. Adjusted odds ratios were 1.44 (95% CI, 0.83-2.49) for moderate-stable, 1.86 (95% CI, 0.91-3.82) for moderate-increasing, 2.28 (95% CI, 1.24-4.18), for elevated-stable, and 3.70 (95% CI, 1.66-8.20) for elevated-increasing groups. The adjusted prevalence of a CAC score of 100 HU or higher was 5.8% in the low-stable group. These odds ratios represent an absolute increase of 2.7%, 5%, 6.3%, and 12.9% for the prevalence of a CAC score of 100 HU or higher for the moderate-stable, moderate-increasing, elevated-stable and elevated-increasing groups, respectively, compared with the low-stable group. Associations were not altered after adjustment for baseline and year 25 BP. Findings were similar for trajectories of isolated systolic BP trajectories but were attenuated for diastolic BP trajectories.
Conclusions and relevance: Blood pressure trajectories throughout young adulthood vary, and higher BP trajectories were associated with an increased risk of CAC in middle age. Long-term trajectories in BP may assist in more accurate identification of individuals with subclinical atherosclerosis.
Conflict of interest statement
Figures
Comment in
-
Early patterns of blood pressure change and future coronary atherosclerosis.JAMA. 2014 Feb 5;311(5):471-2. doi: 10.1001/jama.2013.285123. JAMA. 2014. PMID: 24496535 No abstract available.
References
-
- Vasan RS, Massaro JM, Wilson PW, et al. Antecedent blood pressure and risk of cardiovascular disease: the Framingham Heart Study. Circ. 2002;105(1):48–53. - PubMed
-
- Lee DS, Massaro JM, Wang TJ, et al. Antecedent blood pressure, body mass index, and the risk of incident heart failure in later life. Hypertension. 2007;50(5):869–876. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201300026C/HL/NHLBI NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- AG0005/AG/NIA NIH HHS/United States
- K07 CA154862/CA/NCI NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- HHSN268201300025C/HL/NHLBI NIH HHS/United States
- HHSN268201300027C/HL/NHLBI NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- R01 HL098445/HL/NHLBI NIH HHS/United States
- HHSN268201300029C/HL/NHLBI NIH HHS/United States
- HHSN268200900041C/HL/NHLBI NIH HHS/United States
- HHSN268201300028C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
