

Strategies to improve retention in randomised trials: a Cochrane systematic review and meta-analysis
- PMID: 24496696
- PMCID: PMC3918995
- DOI: 10.1136/bmjopen-2013-003821
Strategies to improve retention in randomised trials: a Cochrane systematic review and meta-analysis
Abstract
Objective: To quantify the effect of strategies to improve retention in randomised trials.
Design: Systematic review and meta-analysis.
Data sources: Sources searched: MEDLINE, EMBASE, PsycINFO, DARE, CENTRAL, CINAHL, C2-SPECTR, ERIC, PreMEDLINE, Cochrane Methodology Register, Current Controlled Trials metaRegister, WHO trials platform, Society for Clinical Trials (SCT) conference proceedings and a survey of all UK clinical trial research units.
Review methods: Included trials were randomised evaluations of strategies to improve retention embedded within host randomised trials. The primary outcome was retention of trial participants. Data from trials were pooled using the fixed-effect model. Subgroup analyses were used to explore the heterogeneity and to determine whether there were any differences in effect by the type of strategy.
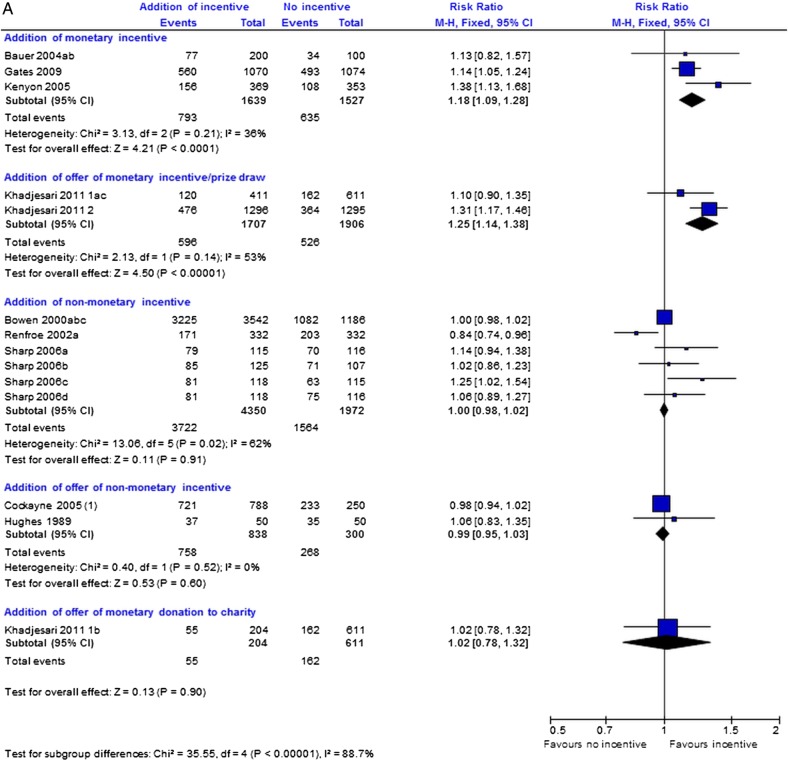
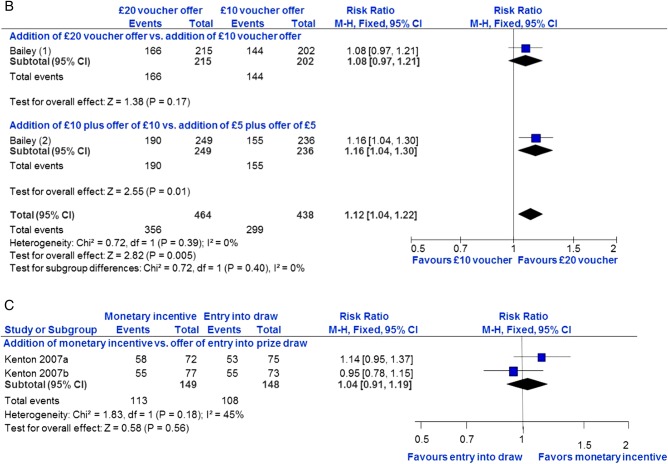
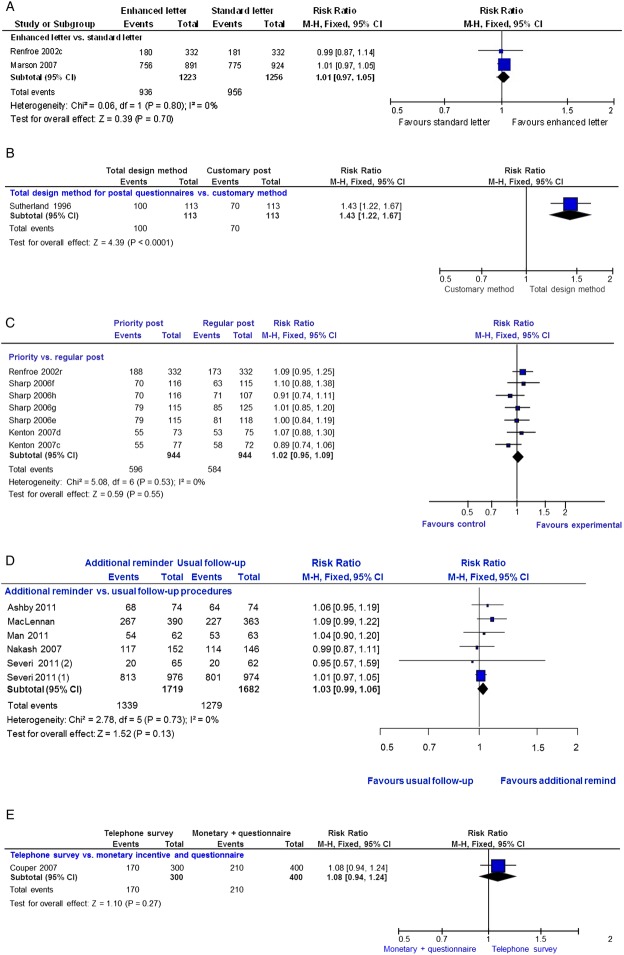
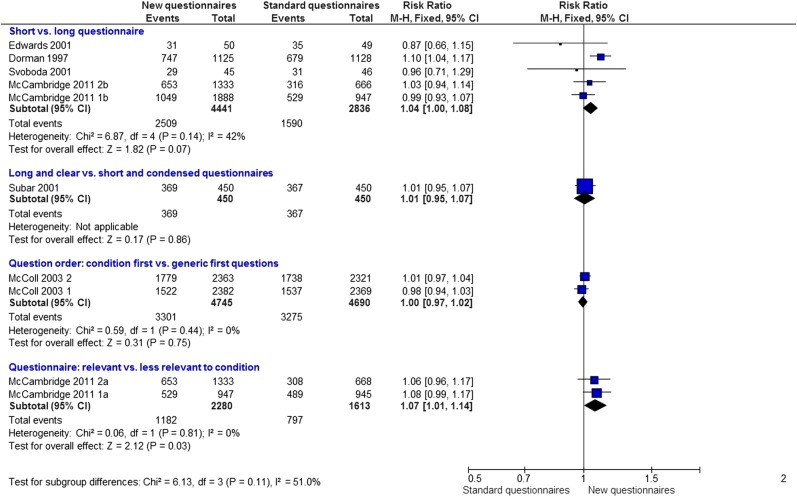
Results: 38 retention trials were identified. Six broad types of strategies were evaluated. Strategies that increased postal questionnaire responses were: adding, that is, giving a monetary incentive (RR 1.18; 95% CI 1.09 to 1.28) and higher valued incentives (RR 1.12; 95% CI 1.04 to 1.22). Offering a monetary incentive, that is, an incentive given on receipt of a completed questionnaire, also increased electronic questionnaire response (RR 1.25; 95% CI 1.14 to 1.38). The evidence for shorter questionnaires (RR 1.04; 95% CI 1.00 to 1.08) and questionnaires relevant to the disease/condition (RR 1.07; 95% CI 1.01 to 1.14) is less clear. On the basis of the results of single trials, the following strategies appeared effective at increasing questionnaire response: recorded delivery of questionnaires (RR 2.08; 95% CI 1.11 to 3.87); a 'package' of postal communication strategies (RR 1.43; 95% CI 1.22 to 1.67) and an open trial design (RR 1.37; 95% CI 1.16 to 1.63). There is no good evidence that the following strategies impact on trial response/retention: adding a non-monetary incentive (RR=1.00; 95% CI 0.98 to 1.02); offering a non-monetary incentive (RR=0.99; 95% CI 0.95 to 1.03); 'enhanced' letters (RR=1.01; 95% CI 0.97 to 1.05); monetary incentives compared with offering prize draw entry (RR=1.04; 95% CI 0.91 to 1.19); priority postal delivery (RR=1.02; 95% CI 0.95 to 1.09); behavioural motivational strategies (RR=1.08; 95% CI 0.93 to 1.24); additional reminders to participants (RR=1.03; 95% CI 0.99 to 1.06) and questionnaire question order (RR=1.00, 0.97 to 1.02). Also based on single trials, these strategies do not appear effective: a telephone survey compared with a monetary incentive plus questionnaire (RR=1.08; 95% CI 0.94 to 1.24); offering a charity donation (RR=1.02, 95% CI 0.78 to 1.32); sending sites reminders (RR=0.96; 95% CI 0.83 to 1.11); sending questionnaires early (RR=1.10; 95% CI 0.96 to 1.26); longer and clearer questionnaires (RR=1.01, 0.95 to 1.07) and participant case management by trial assistants (RR=1.00; 95% CI 0.97 to 1.04).
Conclusions: Most of the trials evaluated questionnaire response rather than ways to improve participants return to site for follow-up. Monetary incentives and offers of monetary incentives increase postal and electronic questionnaire response. Some strategies need further evaluation. Application of these results would depend on trial context and follow-up procedures.
Keywords: Randomised trials; Retention; Strategies.
Figures
References
-
- Fewtrell MS, Kennedy K, Singhal A, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch Dis Child 2008;93:458–61 - PubMed
-
- Schulz KF, Grimes DA. Sample size slippages in randomised trials: exclusions and the lost and wayward. Lancet 2002; 359:781–5 - PubMed
-
- Davis L, Broome M, Cox R. Maximizing retention in community-based clinical trials. J Nurs Scholarsh 2002;34:47–53 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous