

Epidemiology and clinical pathophysiology of uric acid kidney stones
- PMID: 24497296
- PMCID: PMC4696481
- DOI: 10.1007/s40620-013-0034-z
Epidemiology and clinical pathophysiology of uric acid kidney stones
Abstract
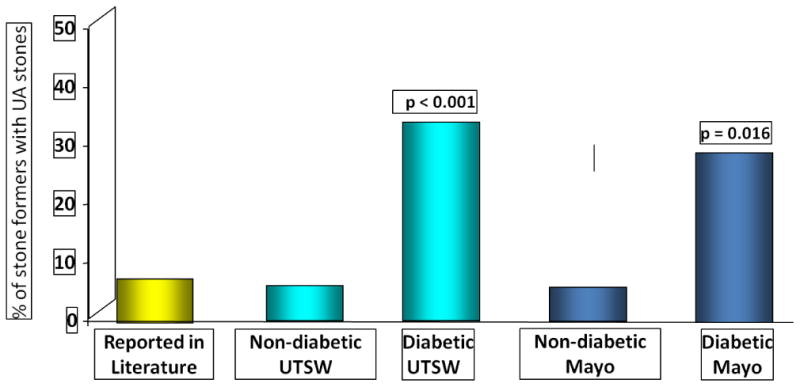
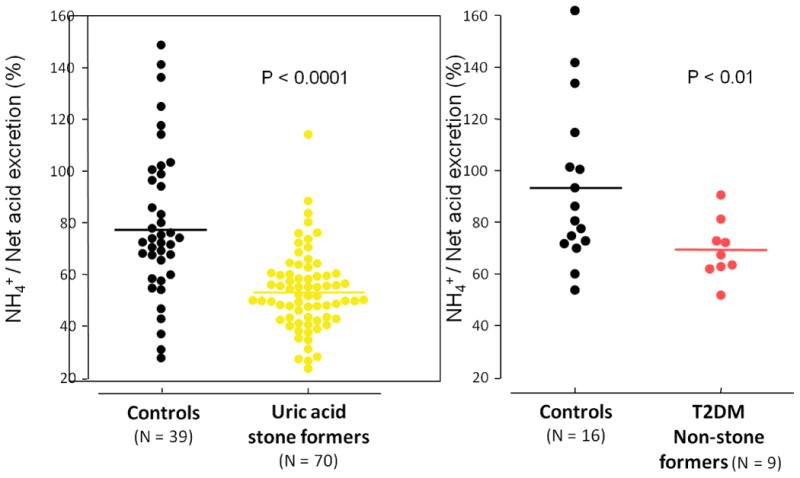
There is global diversity in the prevalence of uric acid (UA) nephrolithiasis. UA nephrolithiasis comprises 8-10 % of all kidney stones in the United States. However, its prevalence is higher in patients with type 2 diabetes mellitus and those with obesity. Three significant urinary abnormalities have been described as the main etiologic factors for the development of UA nephrolithiasis; low urinary pH, hyperuricosuria and low urinary volume. However, an unduly acidic urine below the ionization constant of uric acid (pKa < 5.5) increases the urinary content of undissociated uric acid and thereby uric acid precipitation. Previous studies have shown the two major pathogenic mechanisms for unduly urinary pH are increased net acid excretion (NAE) and reduced renal ammonium (NH4 (+)), with a combination resulting in overly acidic urine. The impaired ammonium excretion has been demonstrated in a steady state in 24-hour urine and also following an oral ammonium chloride (NH4Cl) challenge to amplify ammoniogenic defects in this population. Similar abnormalities have been disclosed in normal populations and also in T2DM populations without kidney stones. To date, the underlying mechanism of increased acid production, source and nature of putative organic acid anions have not been fully elucidated. One plausible mechanism is the production of organic acid by intestinal and aerobic metabolism. This may occur in obese, diabetic and uric acid stone formers due to the differences in gut microflora.
Figures
References
-
- Rafique M, Bhutta RA, Rauf A, Chaudhry IA. Chemical composition of upper renal tract calculi in Multan. J Pak Med Assoc. 2000 May;50(5):145–8. - PubMed
-
- Herbstein FH, Kleeberg J, Shalitin Y, Wartski E, Wielinski S. Chemical and x-ray diffraction analysis of urinary stones in Israel. Isr J Med Sci. 1974 Dec;10(12):1493–9. - PubMed
-
- Hossain RZ, Ogawa Y, Hokama S, Morozumi M, Hatano T. Urolithiasis in Okinawa, Japan: a relatively high prevalence of uric acid stones. Int J Urol. 2003 Aug;10(8):411–5. - PubMed
-
- Sakhaee K. Uric Acid Metabolism and Uric Acid Stones. In: Rao PP J, Kavanagh J, editors. Urinary Tract Stone Disease. Manchester, UK: Springer; 2011. pp. 185–93.
-
- Portis AJ, Hermans K, Culhane-Pera KA, Curhan GC. Stone disease in the Hmong of Minnesota: initial description of a high-risk population. J Endourol. 2004 Nov;18(9):853–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
