

Impact of high power and angle of incidence on prism corrections for visual field loss
- PMID: 24497649
- PMCID: PMC3909527
- DOI: 10.1117/1.OE.53.6.061707
Impact of high power and angle of incidence on prism corrections for visual field loss
Abstract
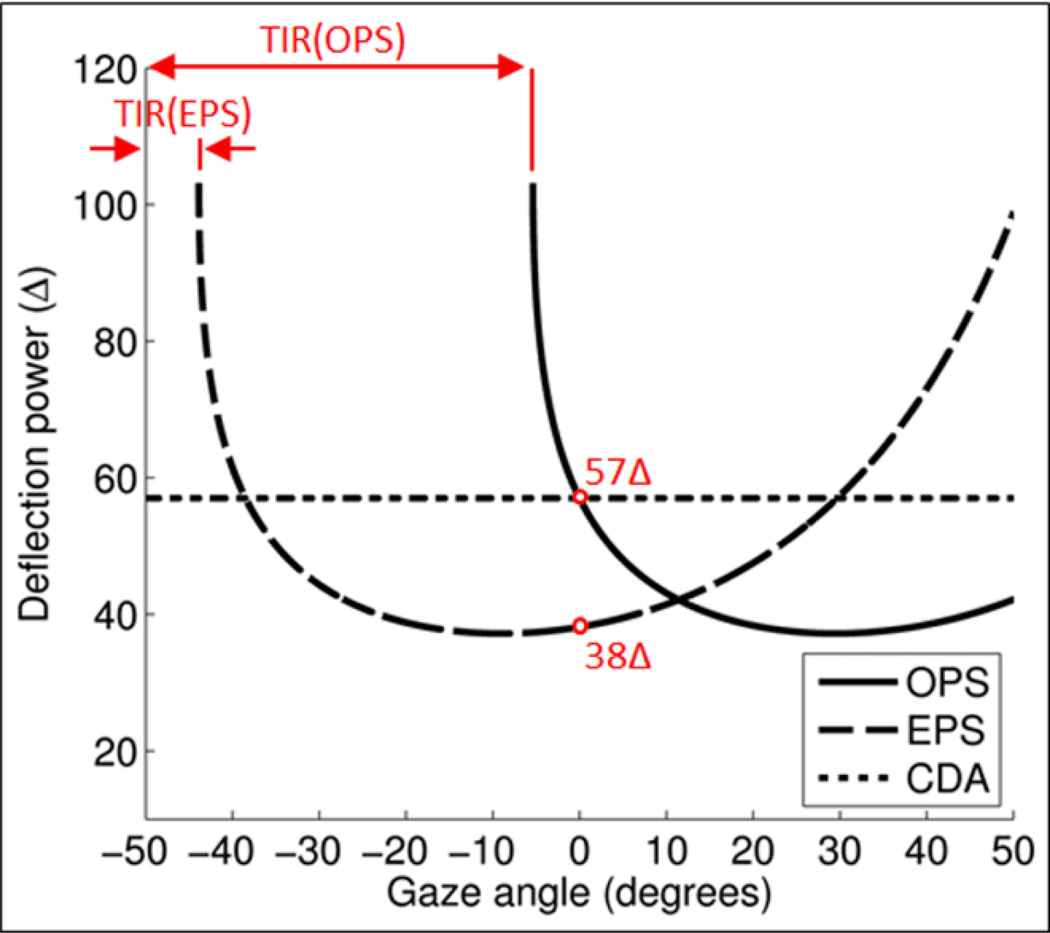
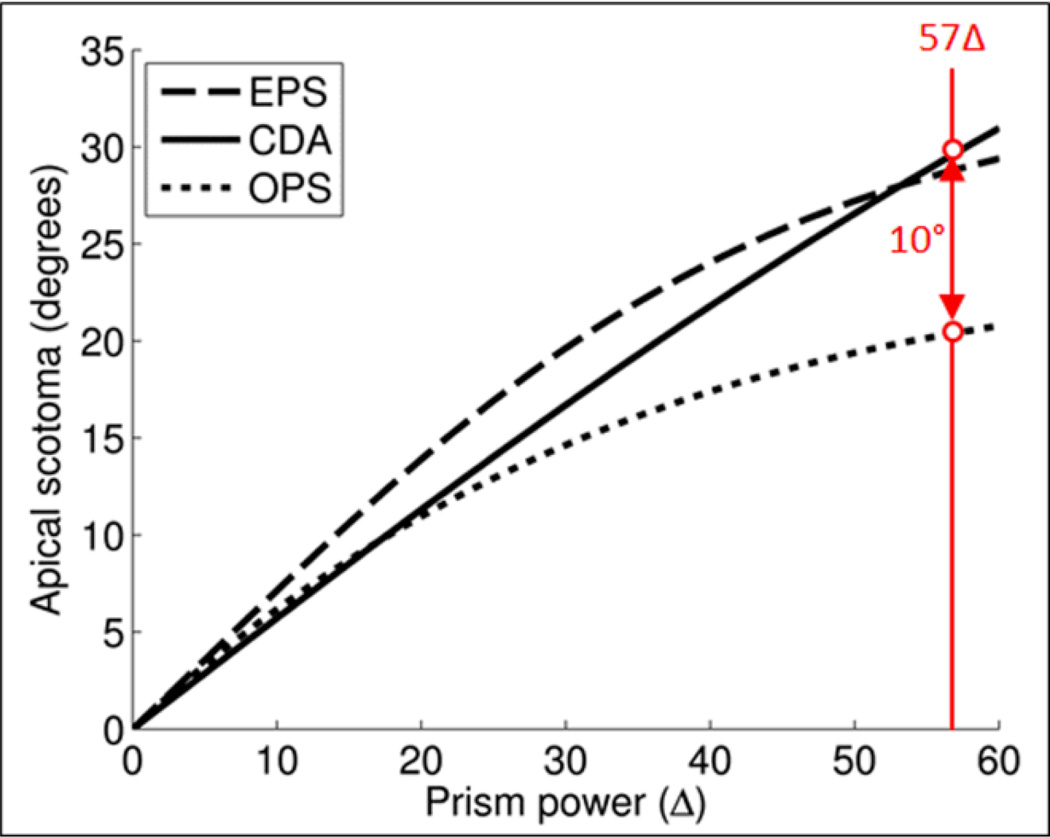
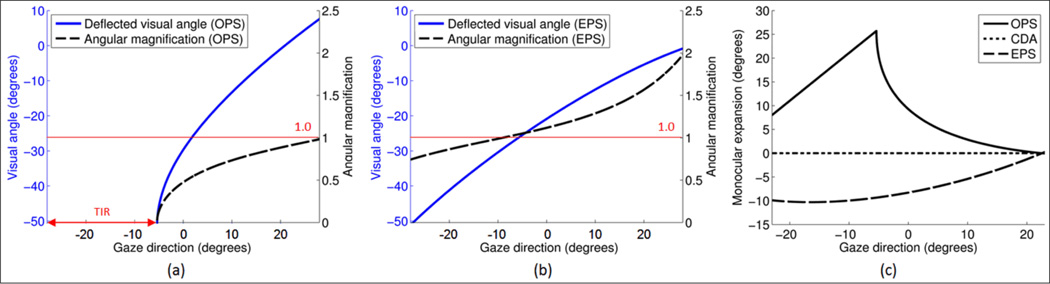
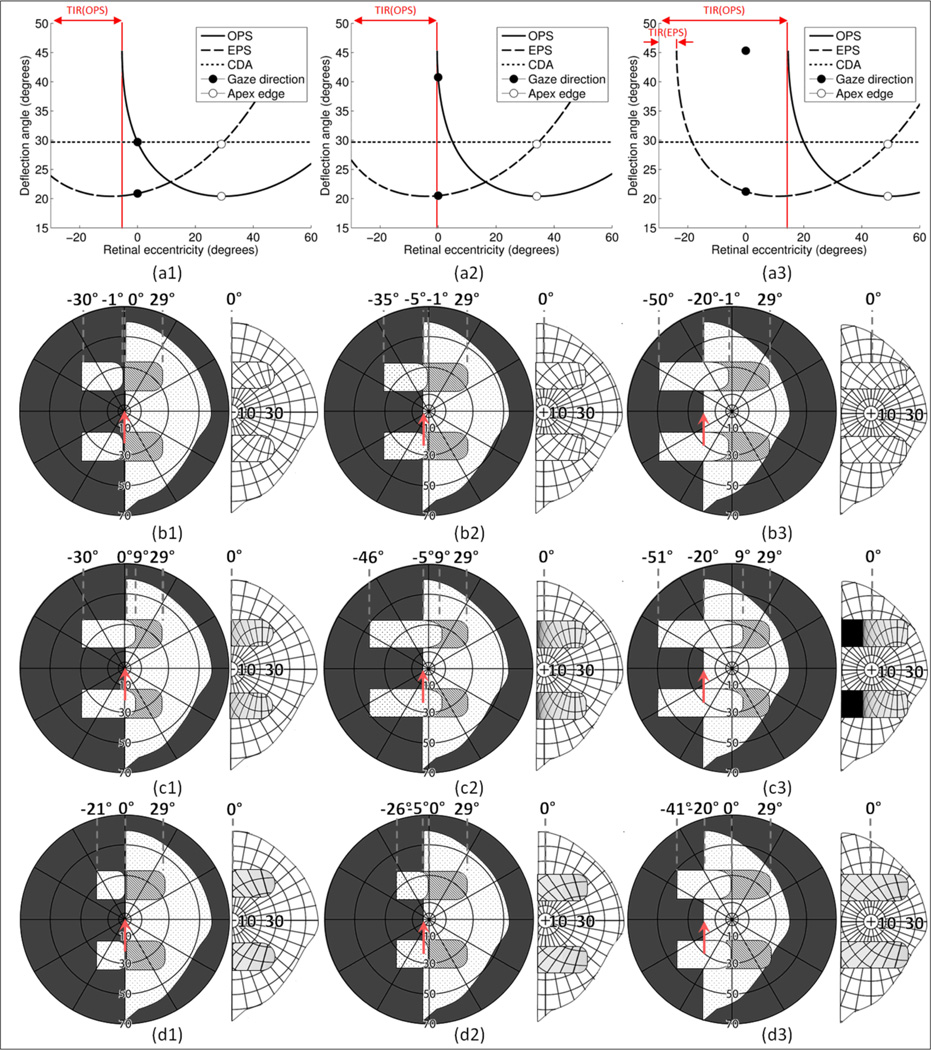
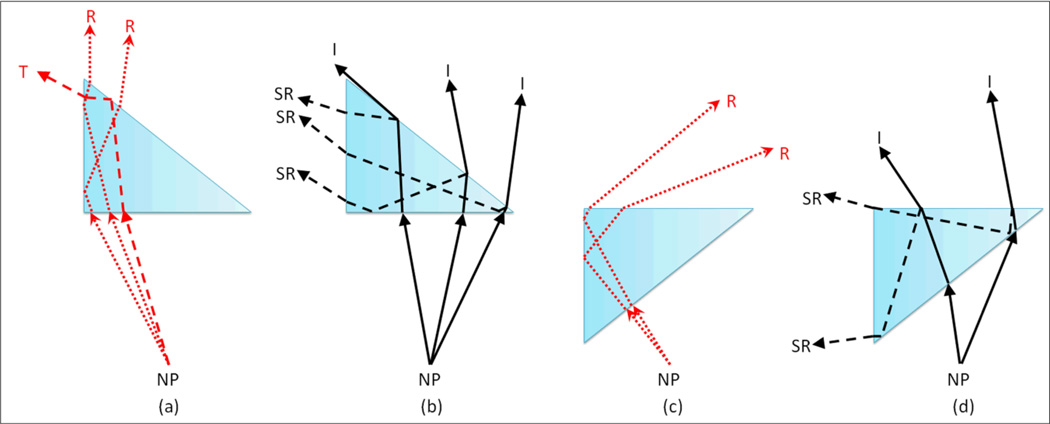
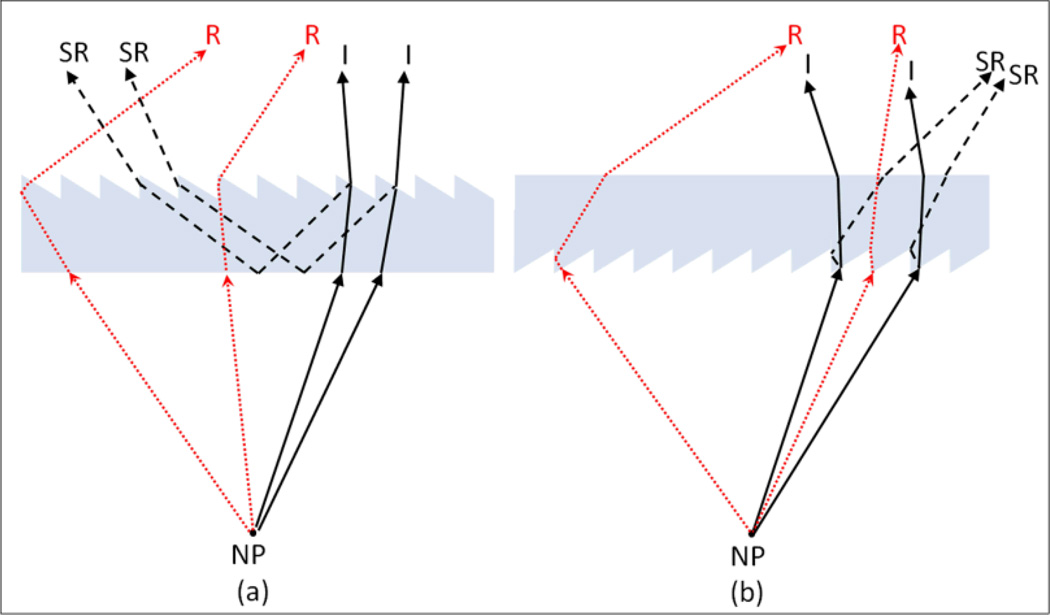
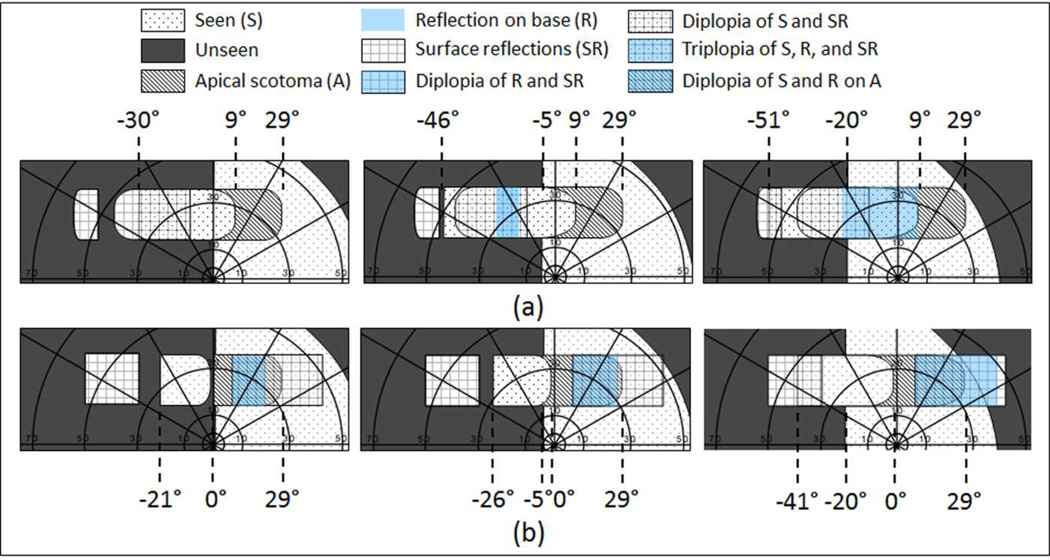
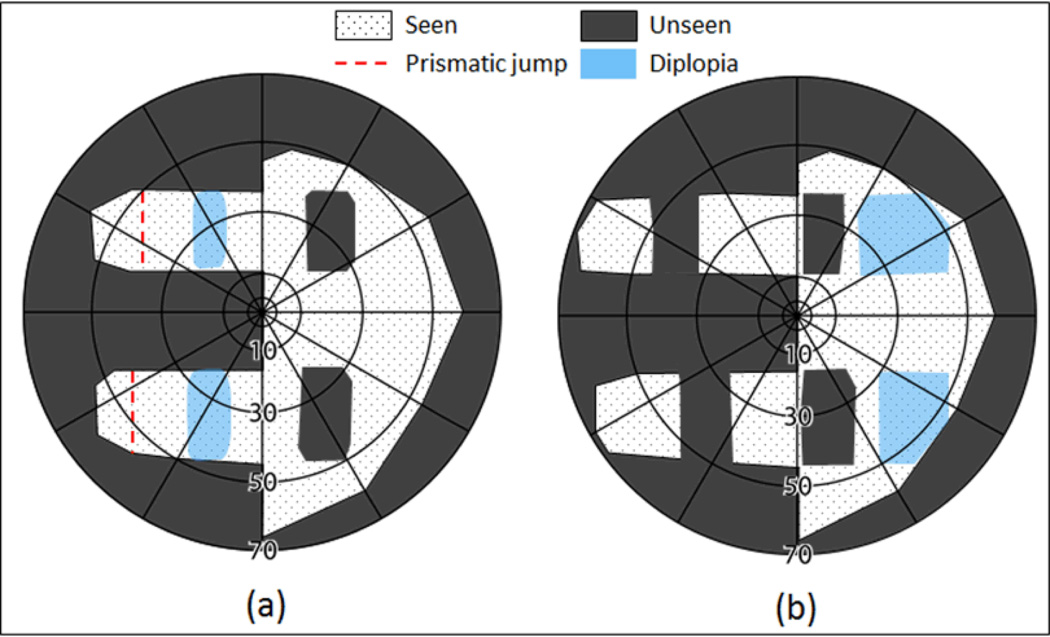
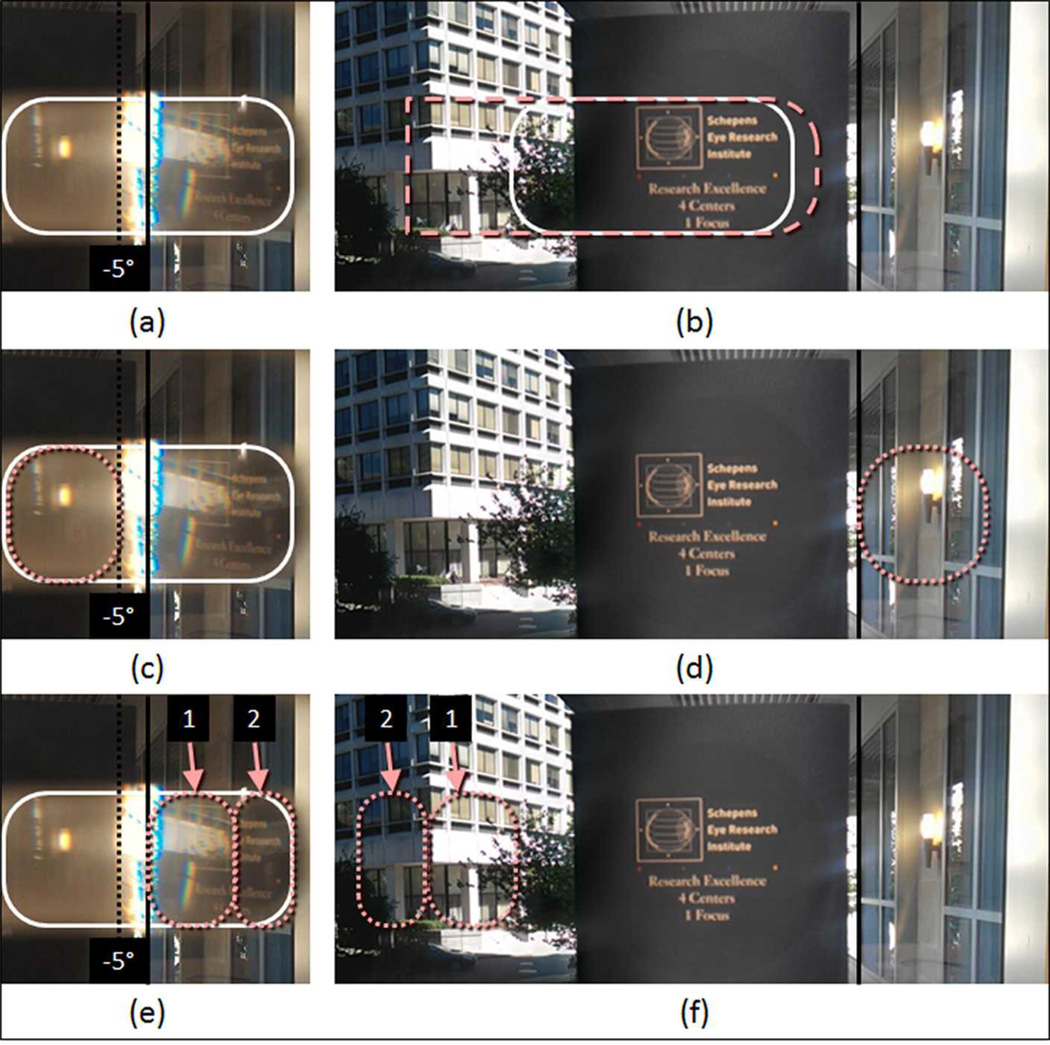
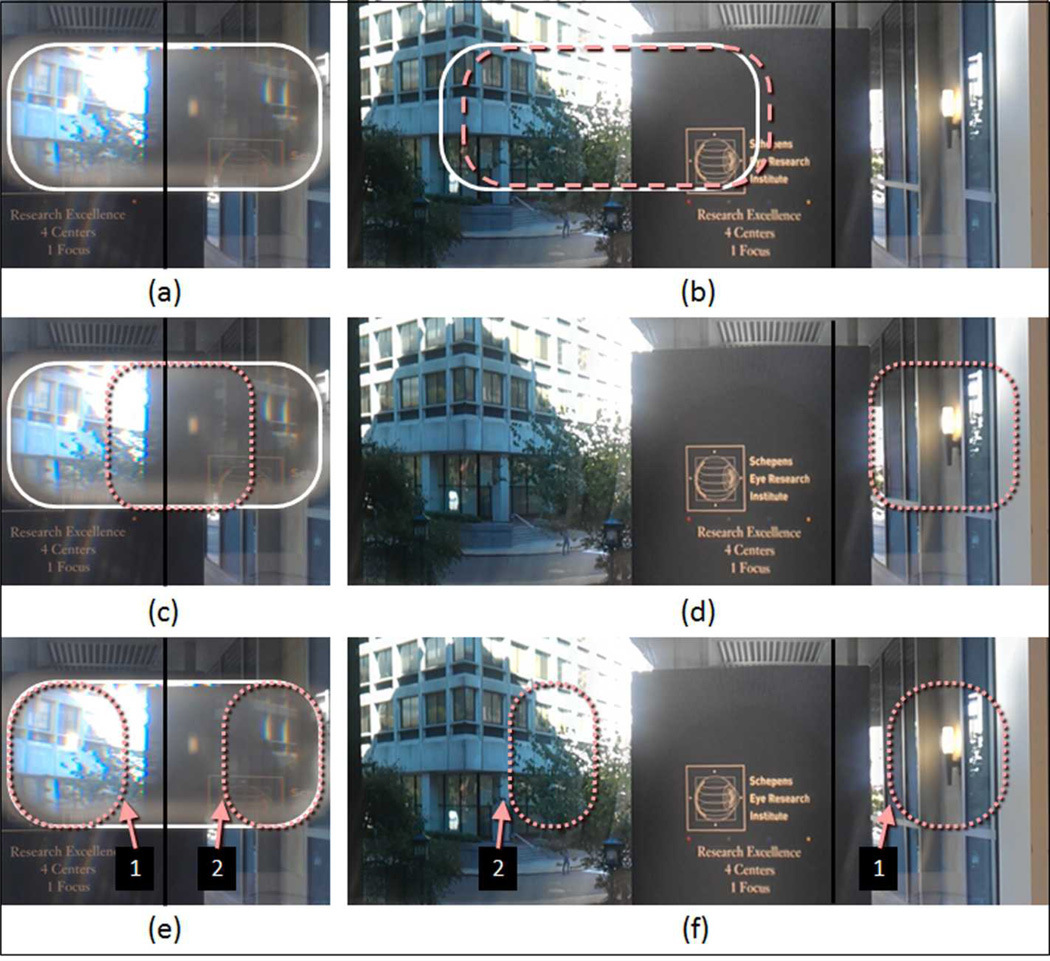
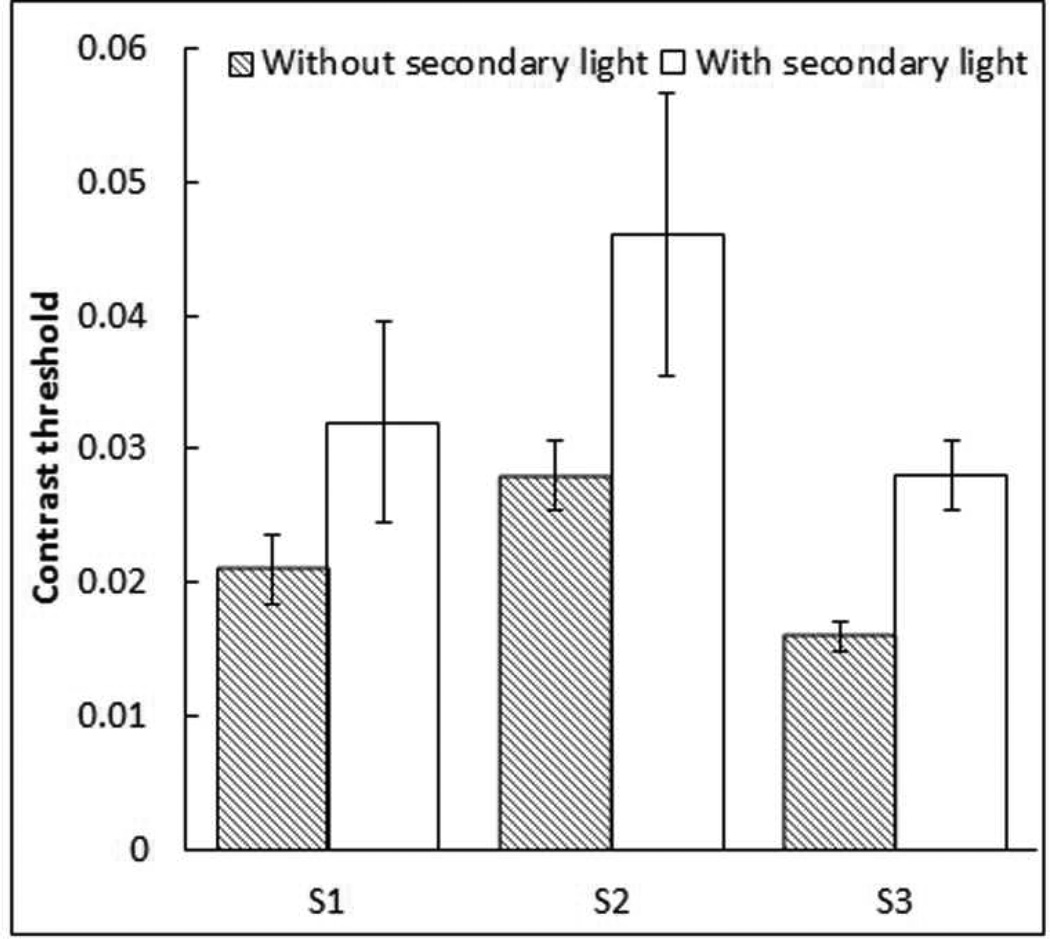
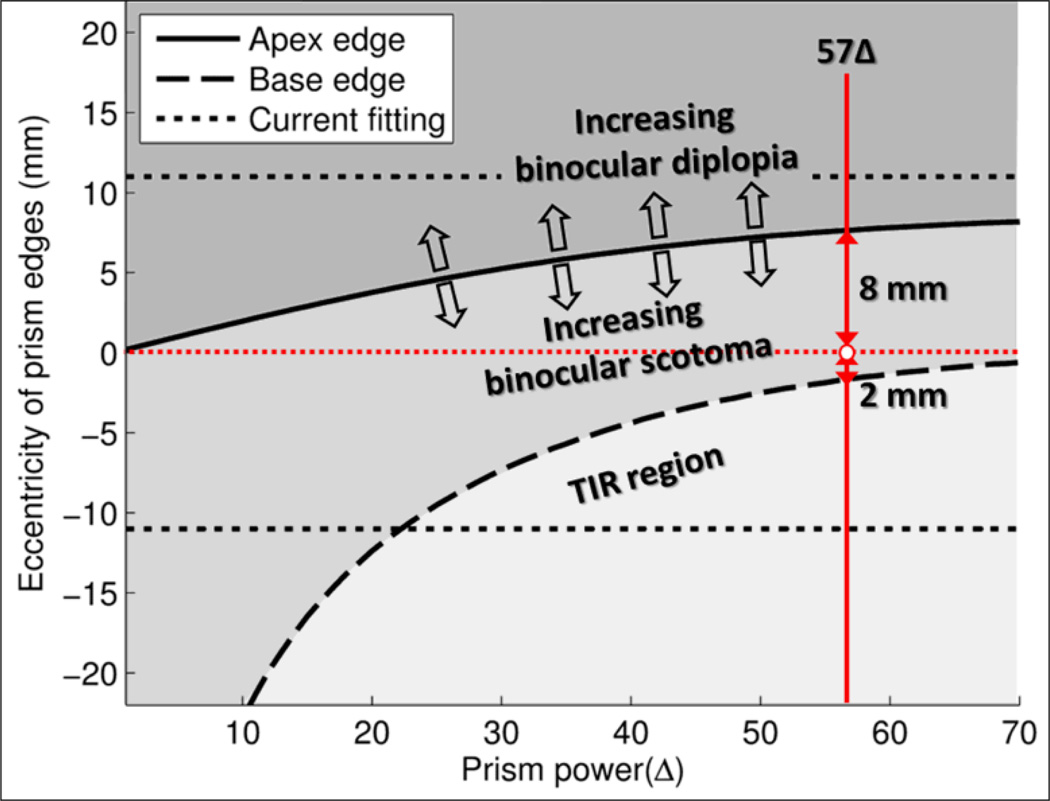
Prism distortions and spurious reflections are not usually considered when prescribing prisms to compensate for visual field loss due to homonymous hemianopia. Distortions and reflections in the high power Fresnel prisms used in peripheral prism placement can be considerable, and the simplifying assumption that prism deflection power is independent of angle of incidence into the prisms results in substantial errors. We analyze the effects of high prism power and incidence angle on the field expansion, size of the apical scotomas, and image compression/expansion. We analyze and illustrate the effects of reflections within the Fresnel prisms, primarily due to reflections at the bases, and secondarily due to surface reflections. The strength and location of these effects differs materially depending on whether the serrated prismatic surface is placed toward or away from the eye, and this affects the contribution of the reflections to visual confusion, diplopia, false alarms, and loss of contrast. We conclude with suggestions for controlling and mitigating these effects in clinical practice.
Keywords: hemianopia; low vision; peripheral prisms; prism distortions; prism treatment; spurious reflections; vision rehabilitation; visual field loss.
Figures
References
-
- Zhang X, Kedar S, Lynn MJ, Newman NJ, Biousse V. Natural history of homonymous hemianopia. Neurology. 2006;66(6):901–905. - PubMed
-
- Rossi PW, Kheyfets S, Reding MJ. Fresnel prisms improve visual perception in stroke patients with homonymous hemianopia or unilateral visual neglect. Neurology. 1990;40(10):1597–1599. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources