

Epidemiology of zoonotic hepatitis E: a community-based surveillance study in a rural population in China
- PMID: 24498033
- PMCID: PMC3909025
- DOI: 10.1371/journal.pone.0087154
Epidemiology of zoonotic hepatitis E: a community-based surveillance study in a rural population in China
Abstract
Background: Hepatitis E is caused by two viral genotype groups: human types and zoonotic types. Current understanding of the epidemiology of the zoonotic hepatitis E disease is founded largely on hospital-based studies.
Methods: The epidemiology of hepatitis E was investigated in a community-based surveillance study conducted over one year in a rural city in eastern China with a registered population of 400,162.
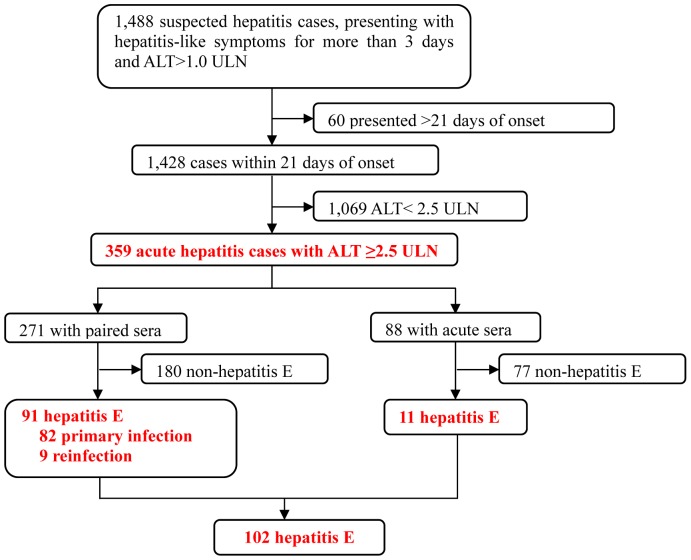
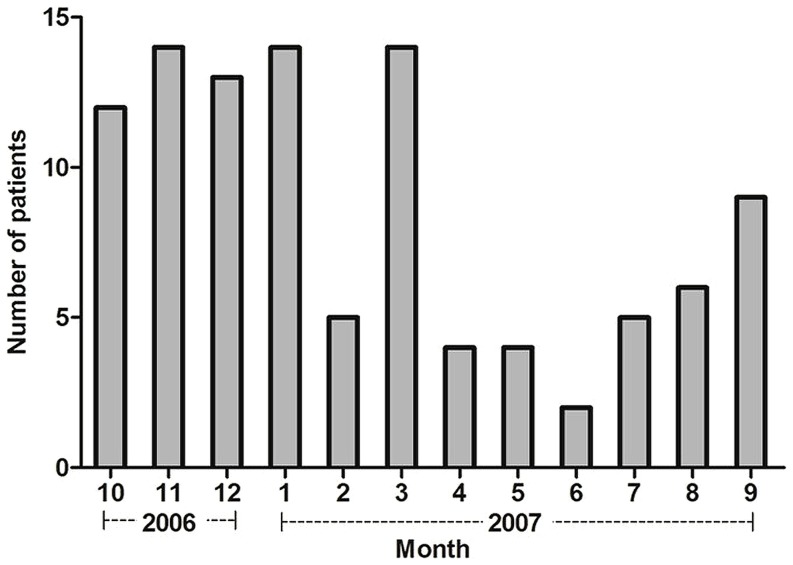
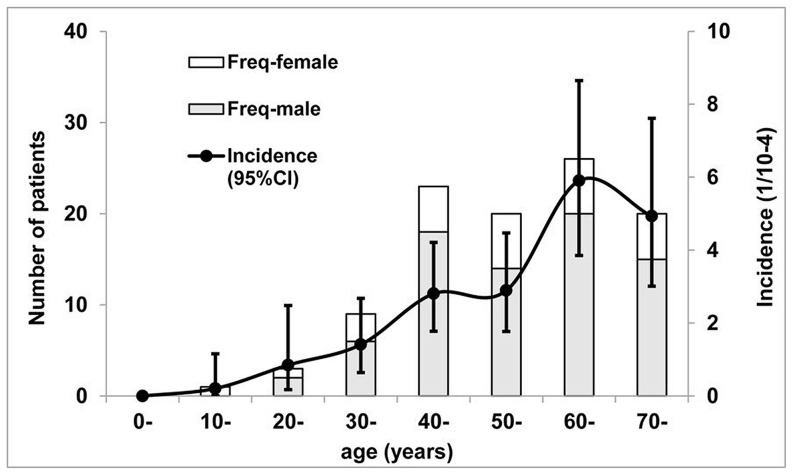
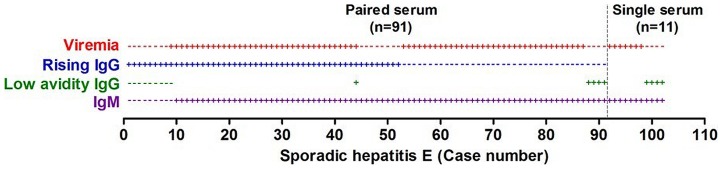
Results: The seroprevalence of hepatitis E in the cohort was 38%. The incidence of hepatitis E was 2.8/10,000 person-years. Totally 93.5% of the infections were attributed to genotype 4 and the rest, to genotype 1. Hepatitis E accounted for 28.4% (102/359) of the acute hepatitis cases and 68.9% (102/148) of the acute viral hepatitis cases in this area of China. The disease occurred sporadically with a higher prevalence during the cold season and in men, with the male-to-female ratio of 3∶1. Additionally, the incidence of hepatitis E increased with age. Hepatitis B virus carriers have an increased risk of contracting hepatitis E than the general population (OR = 2.5, 95%CI 1.5-4.2). Pre-existing immunity to hepatitis E lowered the risk (relative risk = 0.34, 95% CI 0.21-0.55) and reduced the severity of the disease.
Conclusions: Hepatitis E in the rural population of China is essentially that of a zoonosis due to the genotype 4 virus, the epidemiology of which is similar to that due to the other zoonotic genotype 3 virus.
Conflict of interest statement
Figures
References
-
- Purcell RH, Emerson SU (2005) Prevention. In: Thomas HC, Lemon S, Zuckerman AJ, editors. Viral hepatitis, 3rd edn. Malden, MA Blackwell Publishing. pp. 635–645.
-
- Purcell RH, Emerson SU (2008) Hepatitis E: an emerging awareness of an old disease. J Hepatol 48: 494–503. - PubMed
-
- Dalton HR, Bendall RP, Keane FE, Tedder RS, Ijaz S (2009) Persistent carriage of hepatitis E virus in patients with HIV infection. N Engl J Med 361: 1025–1027. - PubMed
-
- Teshale EH, Hu DJ, Holmberg SD (2010) The two faces of hepatitis E virus. Clin Infect Dis 51: 328–334. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
