

Quantification of tortuosity and fractal dimension of the lung vessels in pulmonary hypertension patients
- PMID: 24498123
- PMCID: PMC3909124
- DOI: 10.1371/journal.pone.0087515
Quantification of tortuosity and fractal dimension of the lung vessels in pulmonary hypertension patients
Abstract
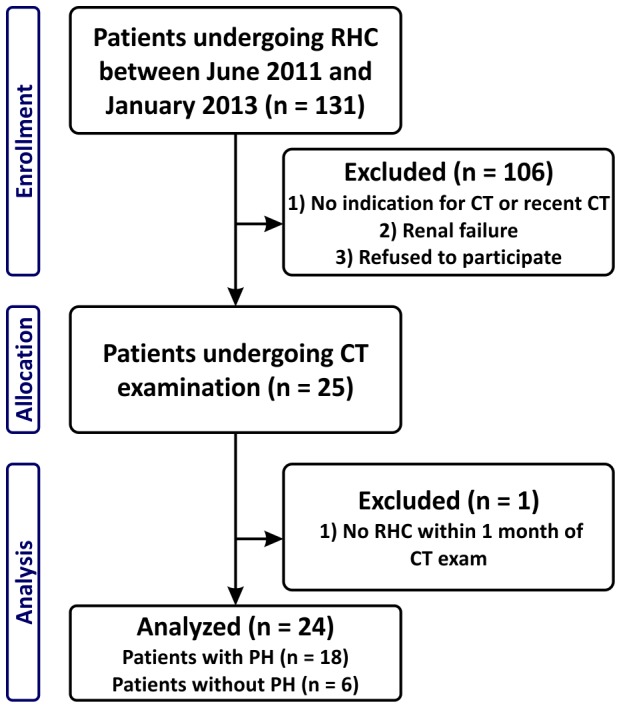
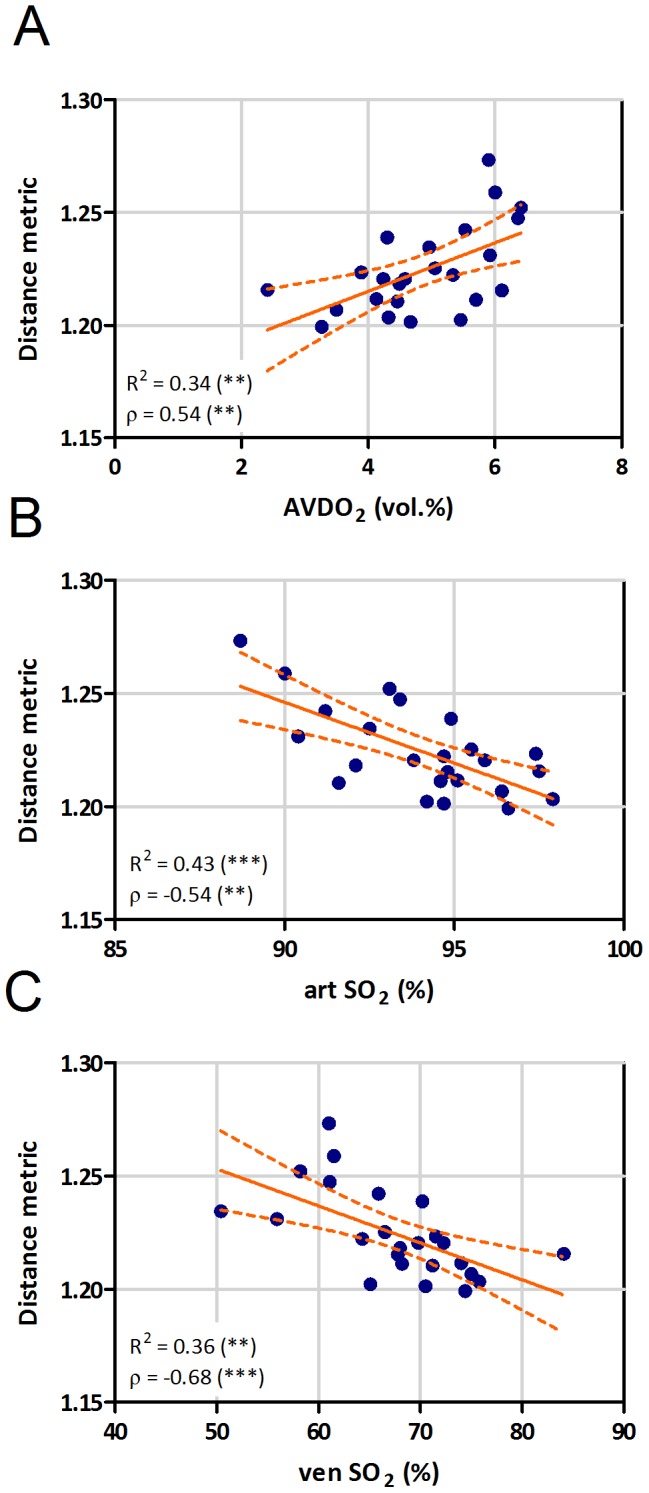
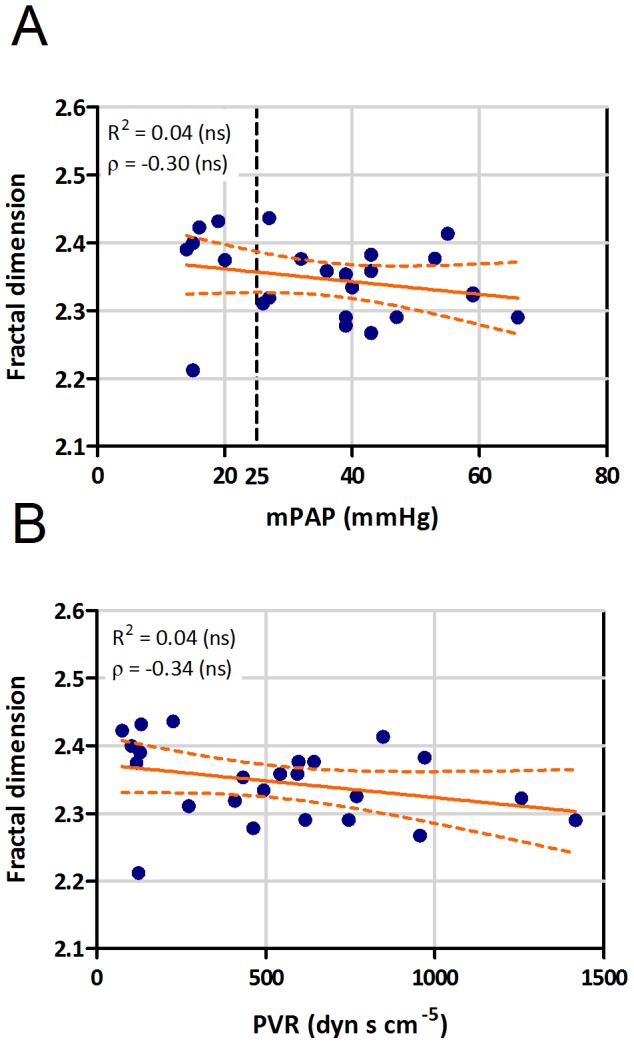
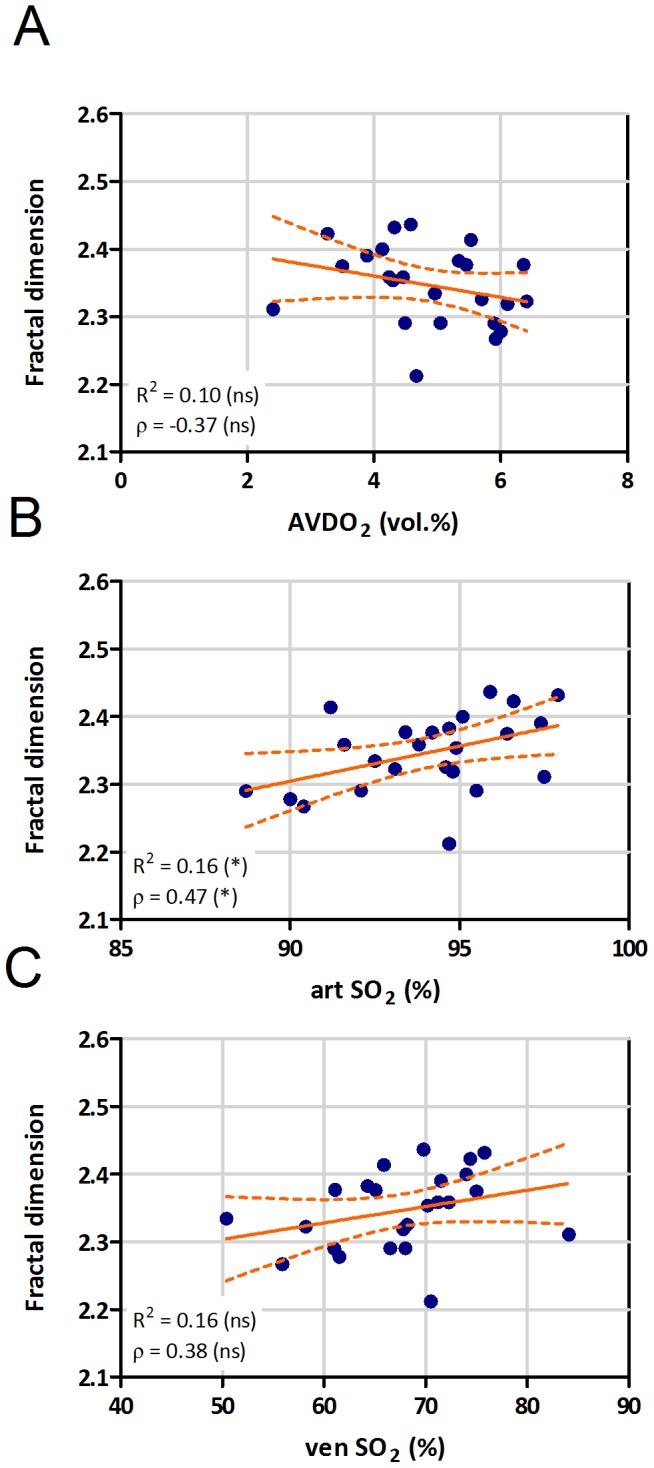
Pulmonary hypertension (PH) can result in vascular pruning and increased tortuosity of the blood vessels. In this study we examined whether automatic extraction of lung vessels from contrast-enhanced thoracic computed tomography (CT) scans and calculation of tortuosity as well as 3D fractal dimension of the segmented lung vessels results in measures associated with PH. In this pilot study, 24 patients (18 with and 6 without PH) were examined with thorax CT following their diagnostic or follow-up right-sided heart catheterisation (RHC). Images of the whole thorax were acquired with a 128-slice dual-energy CT scanner. After lung identification, a vessel enhancement filter was used to estimate the lung vessel centerlines. From these, the vascular trees were generated. For each vessel segment the tortuosity was calculated using distance metric. Fractal dimension was computed using 3D box counting. Hemodynamic data from RHC was used for correlation analysis. Distance metric, the readout of vessel tortuosity, correlated with mean pulmonary arterial pressure (Spearman correlation coefficient: ρ = 0.60) and other relevant parameters, like pulmonary vascular resistance (ρ = 0.59), arterio-venous difference in oxygen (ρ = 0.54), arterial (ρ = -0.54) and venous oxygen saturation (ρ = -0.68). Moreover, distance metric increased with increase of WHO functional class. In contrast, 3D fractal dimension was only significantly correlated with arterial oxygen saturation (ρ = 0.47). Automatic detection of the lung vascular tree can provide clinically relevant measures of blood vessel morphology. Non-invasive quantification of pulmonary vessel tortuosity may provide a tool to evaluate the severity of pulmonary hypertension.
Trial registration: ClinicalTrials.gov NCT01607489.
Conflict of interest statement
Figures


References
-
- Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery J, et al. (2009) Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Resp J 34: 1219–1263. - PubMed
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, et al. (2009) Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 54: S43–S54. - PubMed
-
- Okajima Y, Ohno Y, Washko GR, Hatabu H (2011) Assessment of pulmonary hypertension: What CT and MRI can provide. Acad Radiol 18: 437–453. - PubMed
-
- Stevens GR, Fida N, Sanz J (2012) Computed tomography and cardiac magnetic resonance imaging in pulmonary hypertension. Prog Cardiovasc Dis 55: 161–171. - PubMed
-
- Kulik TJ, Clark RL, Hasan BS, Keane JF, Springmuller D, et al. (2011) Pulmonary arterial hypertension: What the large pulmonary arteries tell us. Pediatr Cardiol 32: 759–765. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
