

Angiotensin-converting enzyme insertion/deletion polymorphism contributes high risk for chronic kidney disease in Asian male with hypertension--a meta-regression analysis of 98 observational studies
- PMID: 24498151
- PMCID: PMC3909221
- DOI: 10.1371/journal.pone.0087604
Angiotensin-converting enzyme insertion/deletion polymorphism contributes high risk for chronic kidney disease in Asian male with hypertension--a meta-regression analysis of 98 observational studies
Abstract
Background: Associations between angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphisms and chronic kidney disease (CKD) have been extensively studied, with most studies reporting that individuals with the D allele have a higher risk. Although some factors, such as ethnicity, may moderate the association between ACE I/D polymorphisms and CKD risk, gender-dependent effects on the CKD risk remain controversial.
Objectives: This study investigated the gender-dependent effects of ACE I/D polymorphisms on CKD risk.
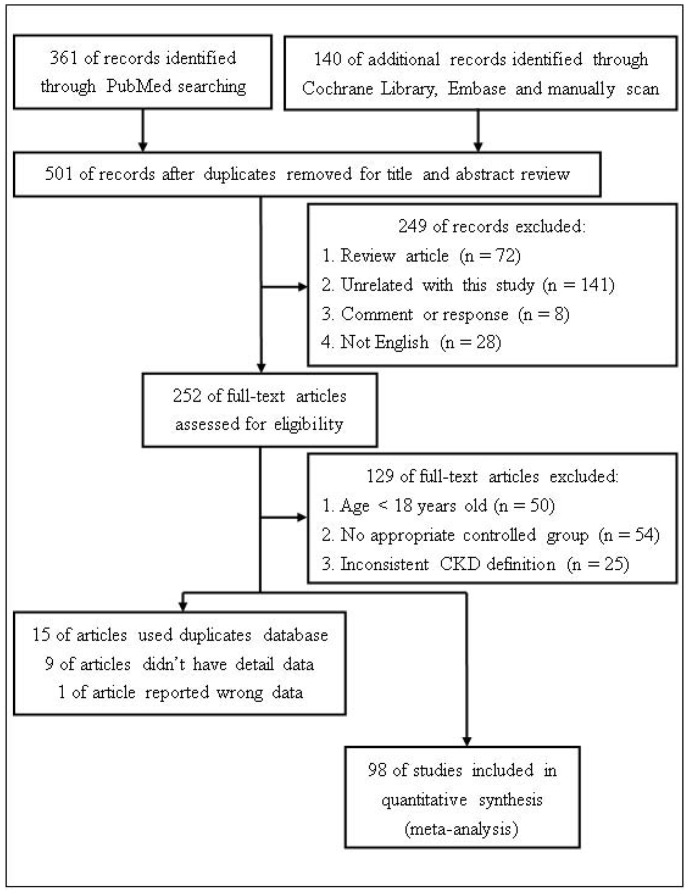
Data sources: PubMed, the Cochrane library, and EMBASE were searched for studies published before January 2013.
Study eligibility criteria participants and interventions: Cross-sectional surveys and case-control studies analyzing ACE I/D polymorphisms and CKD were included. They were required to match the following criteria: age >18 years, absence of rare diseases, and Asian or Caucasian ethnicity.
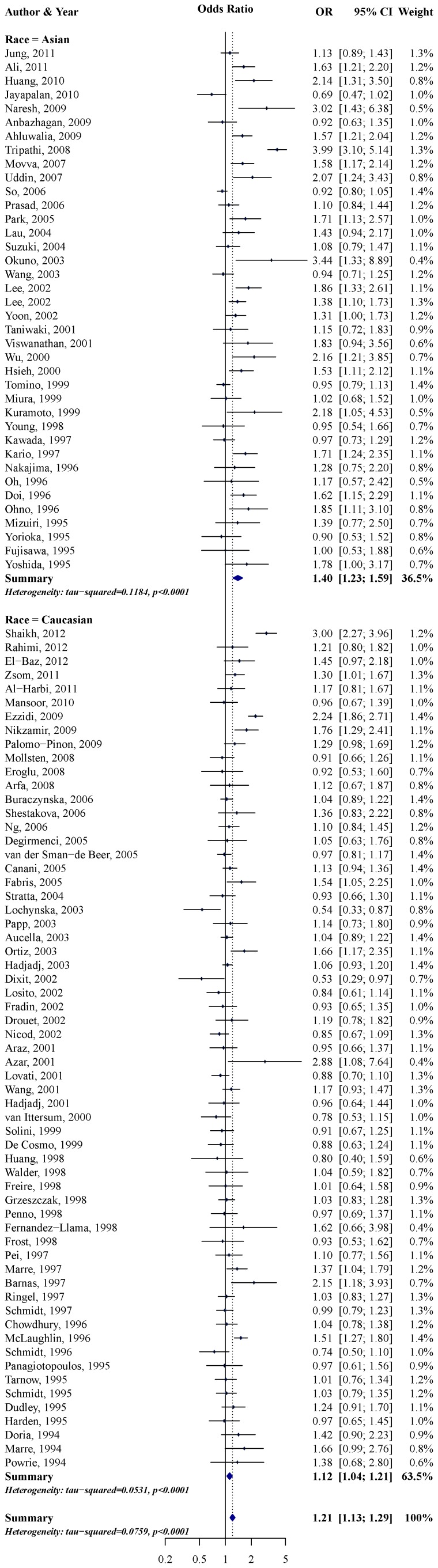
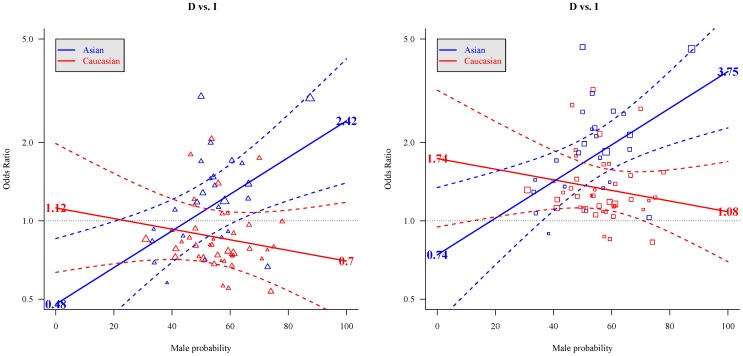
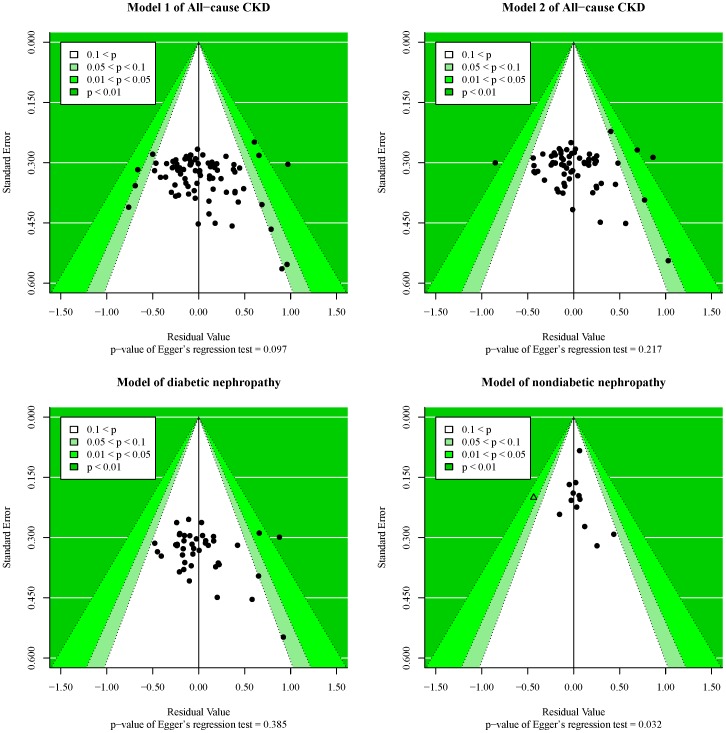
Study appraisal and synthesis methods: The effect of carrying the D allele on CKD risk was assessed by meta-analysis and meta-regression using random-effects models.
Results: ETHNICITY [ODDS RATIO (OR): 1.24; 95% confidence interval (CI): 1.08-1.42] and hypertension (OR: 1.55; 95% CI: 1.04-2.32) had significant moderate effects on the association between ACE I/D polymorphisms and CKD risk, but they were not significant in the diabetic nephropathy subgroup. Males had higher OR for the association between ACE I/D polymorphisms and CKD risk than females in Asians but not Caucasians, regardless of adjustment for hypertension (p<0.05). In subgroup analyses, this result was significant in the nondiabetic nephropathy group. Compared with the I allele, the D allele had the highest risk (OR: 3.75; 95% CI: 1.84-7.65) for CKD in hypertensive Asian males.
Conclusions and implications of key findings: The ACE I/D polymorphisms may incur the highest risk for increasing CKD in hypertensive Asian males.
Conflict of interest statement
Figures
References
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, et al. (2007) Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047. - PubMed
-
- Imai E, Horio M, Watanabe T, Iseki K, Yamagata K, et al. (2009) Prevalence of chronic kidney disease in the Japanese general population. Clin Exp Nephrol 13: 621–630. - PubMed
-
- Zhang L, Wang F, Wang L, Wang W, Liu B, et al. (2012) Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet 379: 815–822. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY (2004) Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305. - PubMed
-
- Li S, McAlpine DD, Liu J, Li S, Collins AJ (2004) Differences between blacks and whites in the incidence of end-stage renal disease and associated risk factors. Adv Ren Replace Ther 11: 5–13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
