

Cost-effectiveness and harm-benefit analyses of risk-based screening strategies for breast cancer
- PMID: 24498285
- PMCID: PMC3911927
- DOI: 10.1371/journal.pone.0086858
Cost-effectiveness and harm-benefit analyses of risk-based screening strategies for breast cancer
Abstract
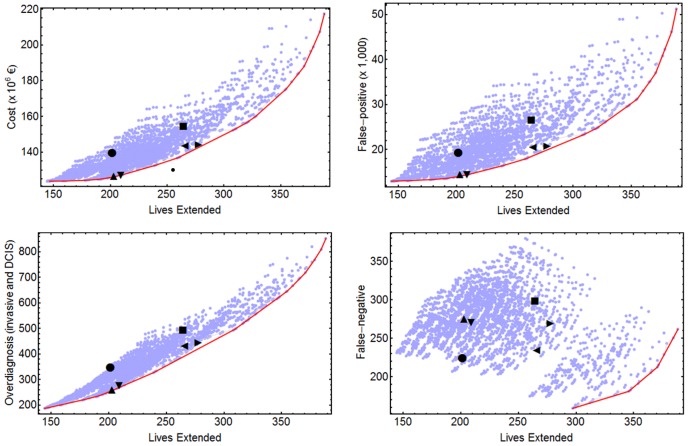
The one-size-fits-all paradigm in organized screening of breast cancer is shifting towards a personalized approach. The present study has two objectives: 1) To perform an economic evaluation and to assess the harm-benefit ratios of screening strategies that vary in their intensity and interval ages based on breast cancer risk; and 2) To estimate the gain in terms of cost and harm reductions using risk-based screening with respect to the usual practice. We used a probabilistic model and input data from Spanish population registries and screening programs, as well as from clinical studies, to estimate the benefit, harm, and costs over time of 2,624 screening strategies, uniform or risk-based. We defined four risk groups, low, moderate-low, moderate-high and high, based on breast density, family history of breast cancer and personal history of breast biopsy. The risk-based strategies were obtained combining the exam periodicity (annual, biennial, triennial and quinquennial), the starting ages (40, 45 and 50 years) and the ending ages (69 and 74 years) in the four risk groups. Incremental cost-effectiveness and harm-benefit ratios were used to select the optimal strategies. Compared to risk-based strategies, the uniform ones result in a much lower benefit for a specific cost. Reductions close to 10% in costs and higher than 20% in false-positive results and overdiagnosed cases were obtained for risk-based strategies. Optimal screening is characterized by quinquennial or triennial periodicities for the low or moderate risk-groups and annual periodicity for the high-risk group. Risk-based strategies can reduce harm and costs. It is necessary to develop accurate measures of individual risk and to work on how to implement risk-based screening strategies.
Conflict of interest statement
Figures

References
-
- Feuer E, Plevritis SK, Berry DA, Cronin KA, editors. et al. The impact of mammography and adjuvant therapy on US breast cancer mortality (1975–2000): collective results from the Cancer Intervention and Surveillance modeling network. J Natl Cancer Inst Monogr 36: 1–126.
-
- Kalager M, Adami HO, Bretthauer M, Tamimi RM (2012) Overdiagnosis of invasive breast cancer due to mammography screening: results from the Norwegian screening program. Ann Intern Med 156: 491–499. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA69976/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- HHSN261201100031C/CA/NCI NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
