

Magnetic resonance imaging criteria to predict complete excision of parasellar pituitary macroadenoma on postoperative imaging
- PMID: 24498588
- PMCID: PMC3912140
- DOI: 10.1055/s-0033-1353362
Magnetic resonance imaging criteria to predict complete excision of parasellar pituitary macroadenoma on postoperative imaging
Abstract
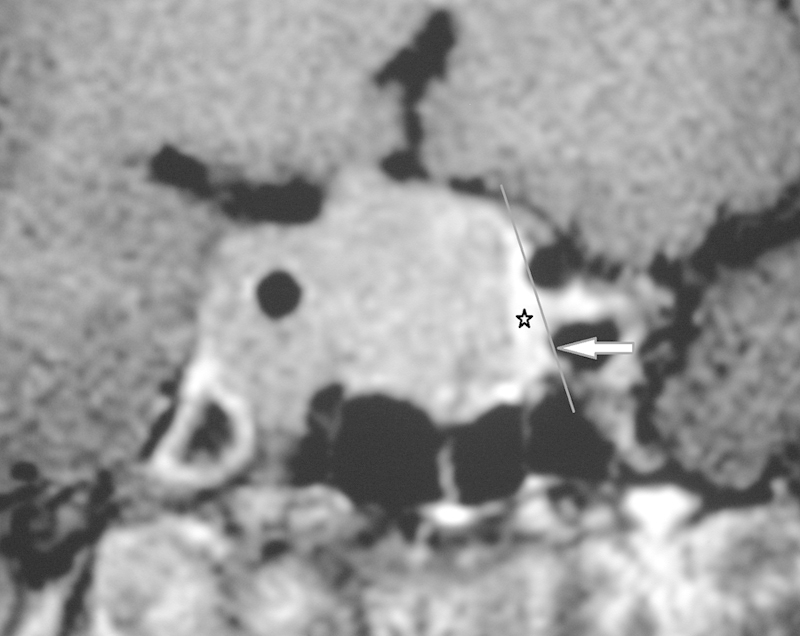
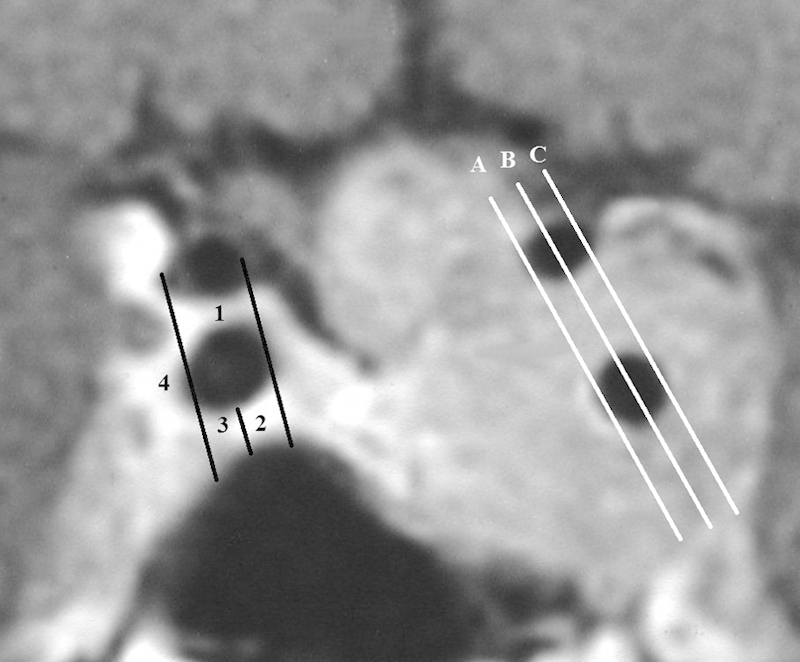
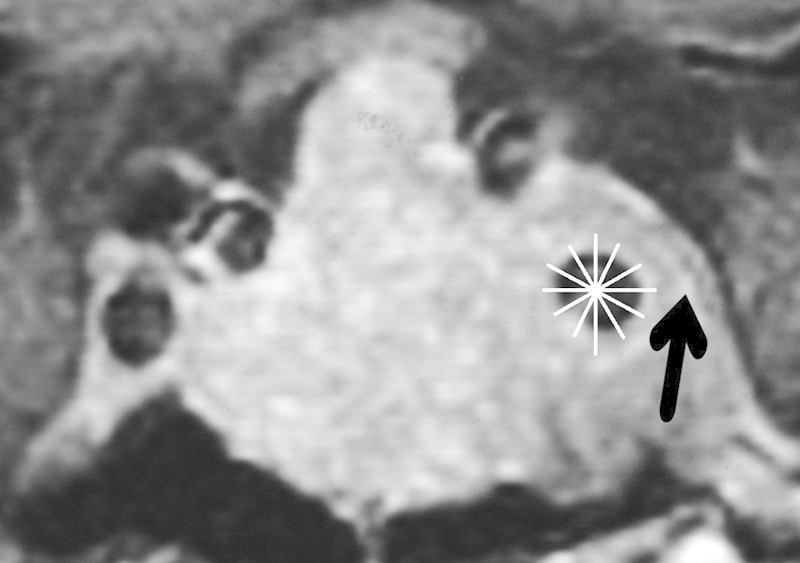
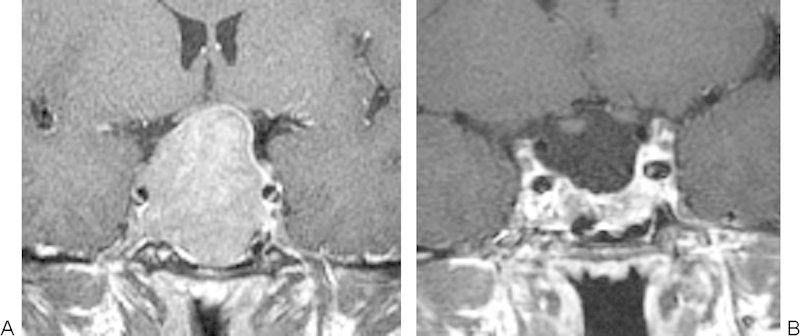
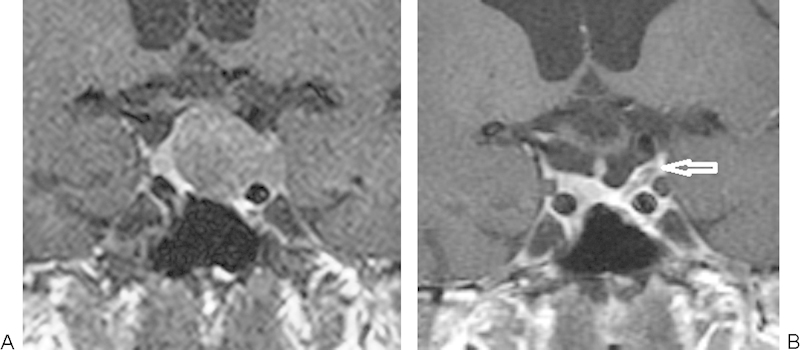
Purpose To evaluate preoperative magnetic resonance imaging (MRI) criteria for their ability to predict the complete removal of parasellar pituitary macroadenoma on the 3-month postoperative MRI. Methods Dedicated pre- and postoperative pituitary MRI studies were reviewed in 49 patients who had undergone transsphenoidal surgery for macroadenomas with potential unilateral parasellar involvement. Twelve preoperative MRI findings and postoperative MRI outcomes were statistically compared. Results Depiction of the inferolateral (positive predictive value [PPV]: 0.6; negative predictive value [NPV], 0.92) and lateral (PPV: 0.65; NPV: 0.85) compartments of the cavernous sinus and the percentage of intracavernous carotid artery encasement (PPV: 0.63; NPV, 1.0 for <50% encasement) were the only criteria significantly predictive of parasellar tumor complete resection. The odds ratios indicated that depiction of the lateral venous or inferolateral venous compartments increased the likelihood of a complete resection by 6 times, whereas for every 25% reduction in intracavernous carotid artery encasement, the chance of a complete resection increased 3.4 times. Conclusion The preoperative MR imaging features that are useful in predicting the complete removal of the parasellar component of a pituitary adenoma as assessed by postoperative MRI are (1) depiction of the lateral and inferolateral compartment of the cavernous sinus and (2) decreasing encasement of the intracavernous carotid artery.
Keywords: macroadenoma; magnetic resonance imaging; pituitary; postoperative.
Figures

References
-
- Alameda C, Lucas T, Pineda E. et al.Experience in management of 51 non-functioning pituitary adenomas: indications for post-operative radiotherapy. J Endocrinol Invest. 2005;28(1):18–22. - PubMed
-
- Ferrante E, Ferraroni M, Castrignanò T. et al.Non-functioning pituitary adenoma database: a useful resource to improve the clinical management of pituitary tumors. Eur J Endocrinol. 2006;155(6):823–829. - PubMed
-
- Greenman Y, Ouaknine G, Veshchev I, Reider-Groswasser I I, Segev Y, Stern N. Postoperative surveillance of clinically nonfunctioning pituitary macroadenomas: markers of tumour quiescence and regrowth. Clin Endocrinol (Oxf) 2003;58(6):763–769. - PubMed
-
- Boelaert K, Gittoes N JL. Radiotherapy for non-functioning pituitary adenomas. Eur J Endocrinol. 2001;144(6):569–575. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
