

Case Reports
doi: 10.1056/NEJMcps1213196.
Clinical problem-solving. Missing elements of the history
- PMID: 24499215
- PMCID: PMC4103154
- DOI: 10.1056/NEJMcps1213196
Item in Clipboard
Case Reports
Clinical problem-solving. Missing elements of the history
N Engl J Med.
.
No abstract available
Conflict of interest statement
Dr. Allen reports receiving consulting fees from Johnson & Johnson, Novartis, Janssen, and Amgen; Dr. Wolfel, lecture fees from Medical Educational Resources; and Dr. Ambardekar, consulting fees from Cytokinetics. No other potential conflict of interest relevant to this article was reported.
Figures
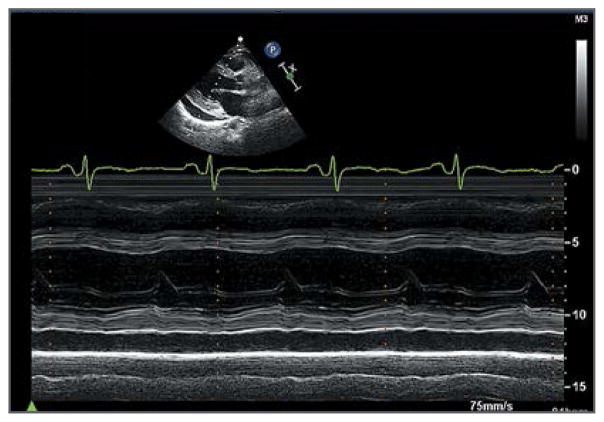
The parasternal long-axis view shows reduced left ventricular systolic function in the absence of left ventricular dilatation or hypertrophy.

Panel A shows a photomicrograph of a specimen of normal myocardium (hematoxylin and eosin) obtained from an autopsy specimen. Panel B shows a photomicrograph of a specimen of the patient’s left ventricular apical core (hematoxylin and eosin) obtained during implantation of a left ventricular assist device for cardiogenic shock. Moderate interstitial, pericellular fibrosis (arrows) and myocyte hypertrophy (arrowheads) are evident. Panel C shows a transmission electron micrograph of an autopsy specimen. Normal myocytes with abundant myofibrils (arrowhead) and morphologically normal mitochondria (asterisk) are present. Panel D shows a transmission electron micrograph of the patient’s left ventricular tissue. Myocytes have degenerative features, characterized by substantial loss of contractile units, intracytoplasmic lipid accumulation (arrows), and lipofuscin deposition (arrowheads). Panel E shows another transmission electron micrograph of the patient’s left ventricular tissue. Both a highly atypical, enlarged mitochondrion (arrowhead) and immediately beneath it several smaller mitochondria (arrows) containing abnormally configured cristae suggest direct mitochondrial injury.
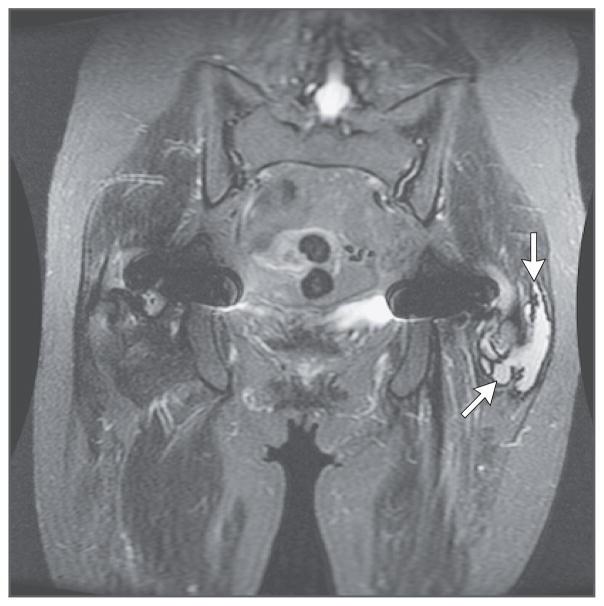
A coronal sagittal short-tau inversion recovery image with arrows pointing to the left pseudotumor is shown. There was a symmetric decrease in muscle mass. A lobular, mildly septated fluid collection posterior to the left greater trochanter, measuring 6.6 cm by 4.2 cm by 1.9 cm, with a thin-walled, well-defined, low-signal rim and no extension into the muscles was suggestive of a metallosis pseudotumor.
Similar articles
-
Initial Experience of Left Ventricular Assist Device Support for Adult Patients with Transposition of the Great Vessels.Congenit Heart Dis. 2015 Sep-Oct;10(5):382-6. doi: 10.1111/chd.12264. Epub 2015 Apr 27. Congenit Heart Dis. 2015. PMID: 25913866 No abstract available.
-
Unusual case of congestive heart failure: cardiac magnetic resonance imaging and histopathologic findings in cobalt cardiomyopathy.Circ Cardiovasc Imaging. 2015 Jun;8(6):e003352. doi: 10.1161/CIRCIMAGING.115.003352. Circ Cardiovasc Imaging. 2015. PMID: 26022382 No abstract available.
-
Percutaneous right ventricular assist device for massive pulmonary embolism.Circ Cardiovasc Interv. 2012 Dec;5(6):e74-5. doi: 10.1161/CIRCINTERVENTIONS.112.973677. Circ Cardiovasc Interv. 2012. PMID: 23250973 No abstract available.
-
A Review of percutaneous mechanical support devices and strategies.Rev Cardiovasc Med. 2018 Mar 30;19(1):21-26. doi: 10.31083/j.rcm.2018.01.904. Rev Cardiovasc Med. 2018. PMID: 31032599 Review.
-
Management of valvulopathies with acute severe heart failure and cardiogenic shock.Arch Cardiovasc Dis. 2019 Dec;112(12):773-780. doi: 10.1016/j.acvd.2019.06.009. Epub 2019 Sep 3. Arch Cardiovasc Dis. 2019. PMID: 31492536 Review.
Cited by
-
Prosthetic hip-associated cobalt toxicity: a systematic review of case series and case reports.EFORT Open Rev. 2022 Mar 17;7(3):188-199. doi: 10.1530/EOR-21-0098. EFORT Open Rev. 2022. PMID: 35298414 Free PMC article. Review.
-
[What entertainment television can do to convey medical knowledge to students and laypeople-raising awareness of rare diseases].Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2021 Jan;64(1):21-27. doi: 10.1007/s00103-020-03259-9. Epub 2020 Dec 9. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2021. PMID: 33296003 Free PMC article. Review. German.
-
The association of cobalturia with cobaltism symptoms a prospective blinded study of 229 post-arthroplasty patients.PLoS One. 2023 Dec 21;18(12):e0295203. doi: 10.1371/journal.pone.0295203. eCollection 2023. PLoS One. 2023. PMID: 38127904 Free PMC article.
-
A Systematic Review of Systemic Cobaltism After Wear or Corrosion of Chrome-Cobalt Hip Implants.J Patient Saf. 2019 Jun;15(2):97-104. doi: 10.1097/PTS.0000000000000220. J Patient Saf. 2019. PMID: 26076080 Free PMC article.
-
Cobalt and Chromium Ion Release in Metal-on-Polyethylene and Ceramic-on-Polyethylene THA: A Simulator Study With Cellular and Microbiological Correlations.J Arthroplasty. 2020 Apr;35(4):1123-1129. doi: 10.1016/j.arth.2019.11.031. Epub 2019 Nov 27. J Arthroplasty. 2020. PMID: 31852609 Free PMC article.
References
-
- Graves SE, Rothwell A, Tucker K, Jacobs JJ, Sedrakyan A. A multinational assessment of metal-on-metal bearings in hip replacement. J Bone Joint Surg Am. 2011;93(Suppl 3):43–7. - PubMed
-
- Ardaugh BM, Graves SE, Redberg RF. The 510(k) ancestry of a metal-on-metal hip implant. N Engl J Med. 2013;368:97–100. - PubMed
-
- Rising JP, Reynolds IS, Sedrakyan A. Delays and difficulties in assessing metal-on-metal hip implants. N Engl J Med. 2012;367(1):e1. - PubMed
-
- Cohen D. How safe are metal-on-metal hip implants? BMJ. 2012;344:e1410. - PubMed
-
- Centeno JA, Pestaner JP, Mullick FG, Virmani R. An analytical comparison of cobalt cardiomyopathy and idiopathic dilated cardiomyopathy. Biol Trace Elem Res. 1996;55:21–30. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical