

Common variable immunodeficiency unmasked by treatment of immune thrombocytopenic purpura with Rituximab
- PMID: 24499503
- PMCID: PMC3776283
- DOI: 10.1186/2052-1839-13-4
Common variable immunodeficiency unmasked by treatment of immune thrombocytopenic purpura with Rituximab
Abstract
Background: Hypogammaglobulinemia may be part of several different immunological or malignant conditions, and its origin is not always obvious. Furthermore, although autoimmune cytopenias are known to be associated with common variable immunodeficiency (CVID) and even may precede signs of immunodeficiency, this is not always recognized. Despite novel insight into the molecular immunology of common variable immunodeficiency, several areas of uncertainty remain. In addition, the full spectrum of immunological effects of the B cell depleting anti-CD20 antibody Rituximab has not been fully explored. To our knowledge this is the first report of development of CVID in a patient with normal immunoglobulin prior to Rituximab treatment.
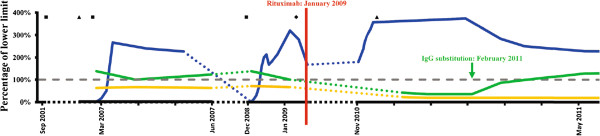
Case presentation: Here we describe the highly unusual clinical presentation of a 34-year old Caucasian male with treatment refractory immune thrombocytopenic purpura and persistent lymphadenopathy, who was splenectomized and received multiple courses of high-dose corticosteroid before treatment with Rituximab resulted in a sustained response. However, in the setting of severe pneumococcal meningitis, hypogammaglobulinemia was diagnosed. An extensive immunological investigation was performed in order to characterize his immune status, and to distinguish between a primary immunodeficiency and a side effect of Rituximab treatment. We provide an extensive presentation and discussion of the literature on the basic immunology of CVID, the mechanism of action of Rituximab, and the immunopathogenesis of hypogammaglobulinemia observed in this patient.
Conclusions: We suggest that CVID should be ruled out in any patient with immune cytopenias in order to avoid diagnostic delay. Likewise, we stress the importance of monitoring immunoglobulin levels before, during, and after Rituximab therapy to identify patients with hypogammaglobulinemia to ensure initiation of immunoglobulin replacement therapy in order to avoid life-threatening invasive bacterial infections. Recent reports indicate that Rituximab is not contra-indicated for the treatment of CVID-associated thrombocytopenia, however concomitant immunoglobulin substitution therapy is of fundamental importance to minimize the risk of infections. Therefore, lessons can be learned from this case report by clinicians caring for patients with immunodeficiencies, haematological diseases or other autoimmune disorders, particularly, when Rituximab treatment may be considered.
Figures
References
-
- Geha RS, Notarangelo LD, Casanova JL, Chapel H, Conley ME, Fischer A. et al. Primary immunodeficiency diseases: an update from the International Union of Immunological Societies Primary Immunodeficiency Diseases Classification Committee. J Allergy Clin Immunol. 2007;120:776–794. doi: 10.1016/j.jaci.2007.08.053. - DOI - PMC - PubMed
-
- Yong PF, Thaventhiran JE, Grimbacher B. "A rose is a rose is a rose," but CVID is Not CVID commonvariable immune deficiency (CVID), what do we know in 2011. Adv Immunol. 2011;111:47–107. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
