

Faecal levels of calprotectin in systemic sclerosis are stable over time and are higher compared to primary Sjögren's syndrome and rheumatoid arthritis
- PMID: 24499541
- PMCID: PMC3978565
- DOI: 10.1186/ar4475
Faecal levels of calprotectin in systemic sclerosis are stable over time and are higher compared to primary Sjögren's syndrome and rheumatoid arthritis
Abstract
Introduction: Faecal calprotectin (FC) has been proposed to be a biomarker of gastrointestinal (GI) disease in systemic sclerosis (SSc). The purpose of this study was to extend cross-sectional observations and prospectively assess the variability of FC over time in SSc patients. We also aimed to examine FC in relation to immunosuppressive therapy. Finally we wanted to analyse FC in other rheumatic diseases to evaluate the specificity of FC for SSc GI disease.
Methods: FC was measured in consecutive patients with SSc, primary Sjögren's syndrome (pSS), rheumatoid arthritis (RA) and in healthy hospital workers. The intraindividual variability of FC in SSc was assessed with intra class correlation (ICC) and κ statistics. Associations between FC and objective markers of GI disease and immunosuppressive medication were investigated.
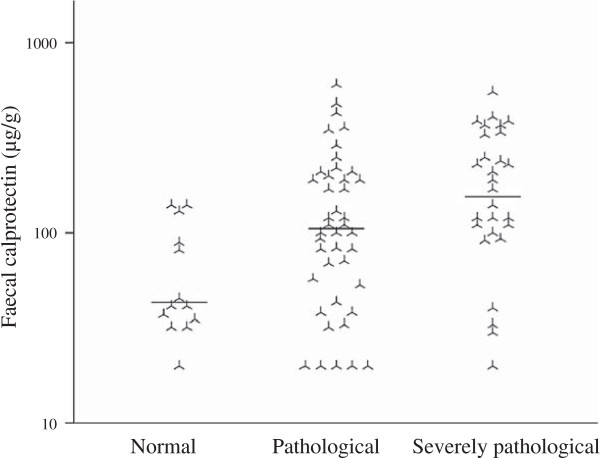
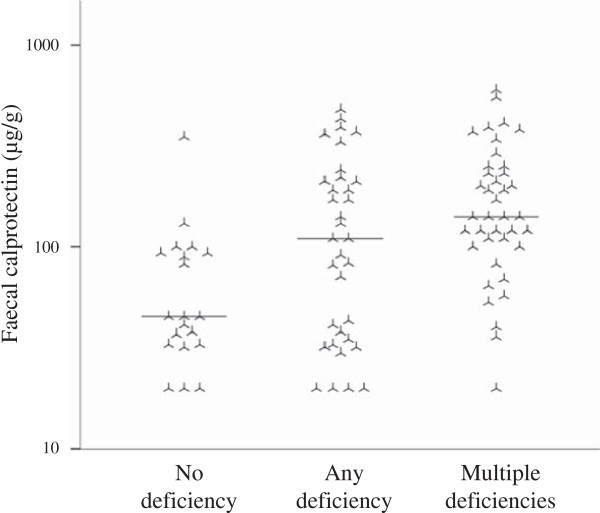
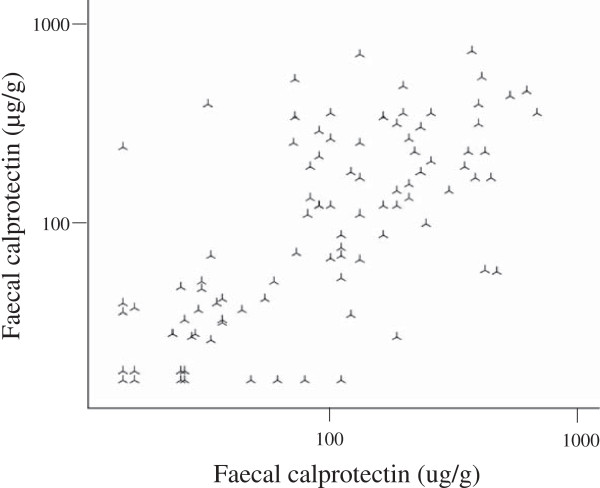
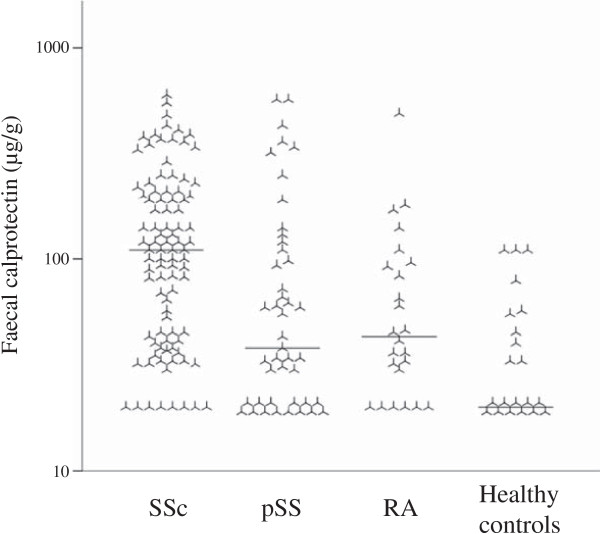
Results: FC was associated with micronutrient deficiency and GI pathology as assessed by cineradiography confirming our previous results. FC showed only a limited intra-individual variation in SSc, ICC = 0.69 (95% confidence interval, CI: 0.57-0.78) and κ = 0.64 (95% CI: 0.56-0.73). Generalised immunosuppression did not have any significant impact on FC. FC was significantly higher in SSc patients compared to patients with pSS or RA as well as compared to healthy subjects.
Conclusions: FC is a promising non-invasive biomarker for GI disease in SSc. In view of stable levels over time, FC could be a useful marker when novel, more specific drugs targeting the GI tract in SSc will be introduced.
Figures
Similar articles
-
Elevated levels of faecal calprotectin in primary Sjögren's syndrome is common and associated with concomitant organic gastrointestinal disease.Arthritis Res Ther. 2016 Jan 12;18:9. doi: 10.1186/s13075-015-0907-8. Arthritis Res Ther. 2016. PMID: 26759247 Free PMC article.
-
Fecal calprotectin in systemic sclerosis and review of the literature.Autoimmun Rev. 2015 Jun;14(6):547-54. doi: 10.1016/j.autrev.2015.01.018. Epub 2015 Feb 4. Autoimmun Rev. 2015. PMID: 25661980 Review.
-
Immunohistochemical characterization of the cellular infiltrates in Sjögren's syndrome, rheumatoid arthritis and osteoarthritis with special reference to calprotectin-producing cells.APMIS. 1996 Dec;104(12):881-90. doi: 10.1111/j.1699-0463.1996.tb04953.x. APMIS. 1996. PMID: 9048866
-
The frequency of sicca symptoms and Sjögren's syndrome in patients with systemic sclerosis.Int J Rheum Dis. 2013 Feb;16(1):88-92. doi: 10.1111/j.1756-185X.2012.01810.x. Epub 2012 Aug 31. Int J Rheum Dis. 2013. PMID: 23441777
-
Sjogren's syndrome is associated with and not secondary to systemic sclerosis.Rheumatology (Oxford). 2007 Feb;46(2):321-6. doi: 10.1093/rheumatology/kel252. Epub 2006 Jul 28. Rheumatology (Oxford). 2007. PMID: 16877466 Review.
Cited by
-
The Role of Fecal Calprotectin in Patients with Systemic Sclerosis and Small Intestinal Bacterial Overgrowth (SIBO).Diagnostics (Basel). 2020 Aug 13;10(8):587. doi: 10.3390/diagnostics10080587. Diagnostics (Basel). 2020. PMID: 32823752 Free PMC article.
-
Update on biomarkers in systemic sclerosis: tools for diagnosis and treatment.Semin Immunopathol. 2015 Sep;37(5):475-87. doi: 10.1007/s00281-015-0506-4. Epub 2015 Jul 14. Semin Immunopathol. 2015. PMID: 26168983 Free PMC article. Review.
-
Soluble Biomarkers for Prediction of Vascular and Gastrointestinal Disease Severity in Patients with Systemic Sclerosis.Curr Treatm Opt Rheumatol. 2021 Mar;7(1):21-38. doi: 10.1007/s40674-021-00171-4. Epub 2021 Feb 11. Curr Treatm Opt Rheumatol. 2021. PMID: 40270643 Free PMC article.
-
Elevated fecal levels of the inflammatory biomarker calprotectin in early systemic sclerosis.Rheumatol Int. 2023 May;43(5):961-967. doi: 10.1007/s00296-022-05264-4. Epub 2022 Dec 25. Rheumatol Int. 2023. PMID: 36566433 Free PMC article.
-
Calprotectin, an available prognostic biomarker in systemic sclerosis: a systematic review.Clin Rheumatol. 2021 May;40(5):1709-1715. doi: 10.1007/s10067-020-05446-0. Epub 2020 Oct 12. Clin Rheumatol. 2021. PMID: 33044726
References
-
- Tibble JA, Bjarnason I. Fecal calprotectin as an index of intestinal inflammation. Drugs Today (Barc) 2001;16:85–96. - PubMed
-
- Tyndall AJ, Bannert B, Vonk M, Airo P, Cozzi F, Carreira PE, Bancel DF, Allanore Y, Müller-Ladner U, Distler O, Iannone F, Pellerito R, Pileckyte M, Miniati I, Ananieva L, Gurman AB, Damjanov N, Mueller A, Valentini G, Riemekasten G, Tikly M, Hummers L, Henriques MJ, Caramaschi P, Scheja A, Rozman B, Ton E, Kumánovics G, Coleiro B, Feierl E. et al.Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann Rheum Dis. 2010;16:1809–1815. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
