

Speech pathologist practice patterns for evaluation and management of suspected cricopharyngeal dysfunction
- PMID: 24500663
- PMCID: PMC4065207
- DOI: 10.1007/s00455-013-9513-6
Speech pathologist practice patterns for evaluation and management of suspected cricopharyngeal dysfunction
Abstract
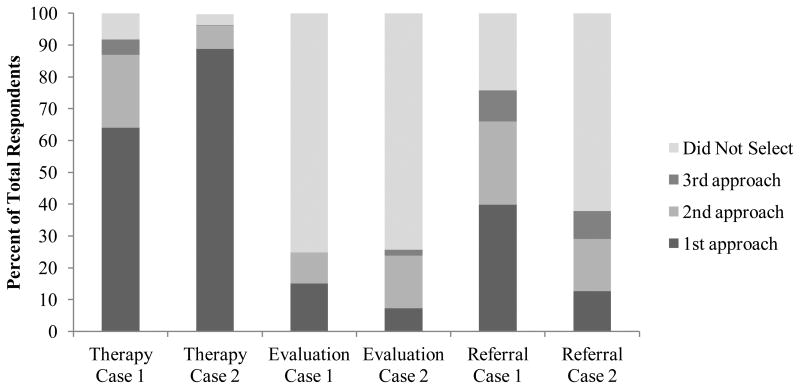
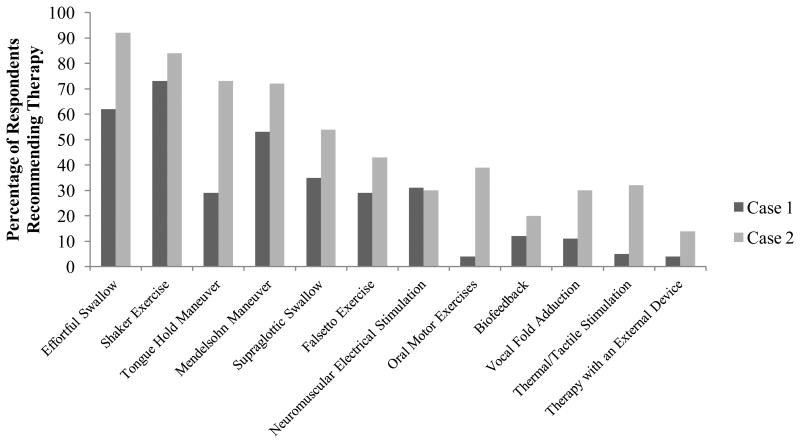
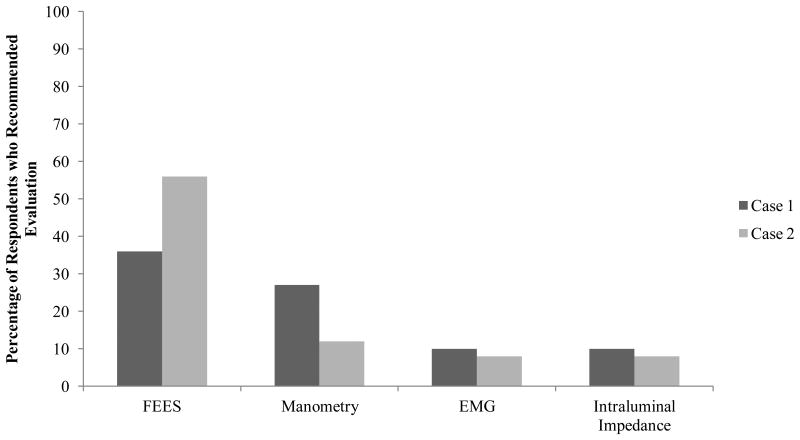
Speech pathologists are often the first professionals to identify signs of a cricopharyngeal (CP) dysfunction and make recommendations for further care. There are many care options for patients with CP dysfunction, but it is unclear how certain interventions are used in practice. A paper-based survey employing two clinical cases involving suspected CP dysfunction (Case 1 with adequate pharyngeal strength and Case 2 with coexisting pharyngeal weakness) was sent to members of American Speech-Language Hearing Association's Special Interest Group 13. Respondents ranked the order of management approaches (swallowing therapy, further evaluation, and referral to another medical professional) and selected specific interventions under each approach that they would recommend for each case. Completed surveys from 206 respondents were entered into analysis. The majority of the respondents recommended swallowing therapy as a first approach for each case (Case 1: 64 %; Case 2: 88 %). The most prevalent swallowing exercises recommended were the Shaker (73 %), effortful swallow (62 %), and Mendelsohn maneuver (53 %) for Case 1 and effortful swallow (92 %), Shaker (84 %), and tongue-hold swallow (73 %) for Case 2. 76 % of respondents recommended a referral for Case 1, while 38 % recommended the same for Case 2. Respondents with access to more types of evaluative tools were more likely to recommend further evaluation, and those with access to only videofluoroscopy were less likely to recommend further evaluation. However, the high degree of variability in recommendations reflects the need for best practice guidelines for patients with signs of CP dysfunction.
Conflict of interest statement
Figures
References
-
- Shaker R, Lang IM. Reflex mediated airway protective mechanisms against retrograde aspiration. Am J Med. 1997;103:64S–73S. - PubMed
-
- Szczesniak MM, Fuentealba SE, Burnett A, Cook IJ. Differential relaxation and contractile responses of the human upper esophageal sphincter mediated by interplay of mucosal and deep mechanoreceptor activation. Am J Physiol Gastrointest Liver Physiol. 2008;294:G982–988. - PubMed
-
- Chernichenko N, Woo JS, Hundal JS, Sasaki CT. Response of cricopharyngeus muscle to esophageal stimulation by mechanical distension and acid and bile perfusion. Ann Otol Rhinol Laryngol. 2011;120:137–142. - PubMed
-
- Ghosh SK, Pandolfino JE, Zhang Q, Jarosz A, Kahrilas PJ. Deglutitive upper esophageal sphincter relaxation: a study of 75 volunteer subjects using solid-state high-resolution manometry. American Journal of Physiology-Gastrointestinal and Liver Physiology. 2006;291:G525–G531. - PubMed
-
- Butler SG, Stuart A, Castell D, Russell GB, Koch K, Kemp S. Effects of Age, Gender, Bolus Condition, Viscosity, and Volume on Pharyngeal and Upper Esophageal Sphincter Pressure and Temporal Measurements During Swallowing. Journal of Speech Language and Hearing Research. 2009;52:240–253. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
