

Tumor dormancy: potential therapeutic target in tumor recurrence and metastasis prevention
- PMID: 24502434
- PMCID: PMC4176492
- DOI: 10.1186/2162-3619-2-29
Tumor dormancy: potential therapeutic target in tumor recurrence and metastasis prevention
Abstract
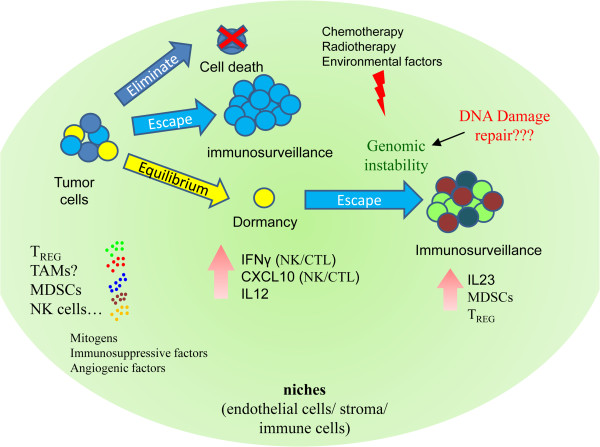
In past decades, cancer patient survival has been improved with earlier detection and advancements in therapy. However, many patients who exhibit no clinical symptoms after frontline therapy subsequently suffer, often many years later, aggressive tumor recurrence. Cancer recurrence represents a critical clinical challenge in effectively treating malignancies and for patients' quality of life. Tumor cell dormancy may help to explain treatment resistance and recurrence or metastatic reactivation. Understanding the dormant stage of tumor cells may help in discovering ways to maintain the dormant state or permanently eliminate dormant residual disseminated tumor cells. Over the past decade, numerous studies indicate that various mechanisms of tumor dormancy exist, including cellular dormancy (quiescence), angiogenic dormancy, and immunologic dormancy. In this short review, we summarize recent experimental and clinical evidence for these three mechanisms and other possible tumor microenvironment mechanisms that may influence tumor dormancy.
Figures



Similar articles
-
Metastatic Cell Dormancy and Re-activation: An Overview on Series of Molecular Events Critical for Cancer Relapse.Anticancer Agents Med Chem. 2017;17(4):472-482. doi: 10.2174/1871520616666160901145857. Anticancer Agents Med Chem. 2017. PMID: 27592547 Review.
-
Regulation of Metastatic Tumor Dormancy and Emerging Opportunities for Therapeutic Intervention.Int J Mol Sci. 2022 Nov 11;23(22):13931. doi: 10.3390/ijms232213931. Int J Mol Sci. 2022. PMID: 36430404 Free PMC article. Review.
-
Cancer cell dormancy: mechanisms and implications of cancer recurrence and metastasis.Onco Targets Ther. 2017 Oct 27;10:5219-5228. doi: 10.2147/OTT.S140854. eCollection 2017. Onco Targets Ther. 2017. PMID: 29138574 Free PMC article. Review.
-
Unveiling cancer dormancy: Intrinsic mechanisms and extrinsic forces.Cancer Lett. 2024 Jun 1;591:216899. doi: 10.1016/j.canlet.2024.216899. Epub 2024 Apr 21. Cancer Lett. 2024. PMID: 38649107 Review.
-
[Mechanisms and implications of cancer cell dormancy in head and neck carcinoma].Hua Xi Kou Qiang Yi Xue Za Zhi. 2018 Feb 1;36(1):92-98. doi: 10.7518/hxkq.2018.01.018. Hua Xi Kou Qiang Yi Xue Za Zhi. 2018. PMID: 29595004 Free PMC article. Chinese.
Cited by
-
The role of vascular endothelial growth factor, interleukin 8, and insulinlike growth factor in sustaining autophagic DIRAS3-induced dormant ovarian cancer xenografts.Cancer. 2019 Apr 15;125(8):1267-1280. doi: 10.1002/cncr.31935. Epub 2019 Jan 8. Cancer. 2019. PMID: 30620384 Free PMC article.
-
Radioresistance in rhabdomyosarcomas: Much more than a question of dose.Front Oncol. 2022 Sep 29;12:1016894. doi: 10.3389/fonc.2022.1016894. eCollection 2022. Front Oncol. 2022. PMID: 36248991 Free PMC article. Review.
-
TFF3 facilitates dormancy of anti-estrogen treated ER+ mammary carcinoma.Commun Med (Lond). 2025 Feb 21;5(1):45. doi: 10.1038/s43856-024-00710-9. Commun Med (Lond). 2025. PMID: 39984660 Free PMC article.
-
The Cross Talk between Cancer Stem Cells/Cancer Initiating Cells and Tumor Microenvironment: The Missing Piece of the Puzzle for the Efficient Targeting of these Cells with Immunotherapy.Cancer Microenviron. 2019 Dec;12(2-3):133-148. doi: 10.1007/s12307-019-00233-1. Epub 2019 Nov 22. Cancer Microenviron. 2019. PMID: 31758404 Free PMC article.
-
Metabolic Plasticity in Ovarian Cancer Stem Cells.Cancers (Basel). 2020 May 17;12(5):1267. doi: 10.3390/cancers12051267. Cancers (Basel). 2020. PMID: 32429566 Free PMC article.
References
-
- Meng S, Tripathy D, Frenkel EP, Shete S, Naftalis EZ, Huth JF, Beitsch PD, Leitch M, Hoover S, Euhus D, Haley B, Morrison L, Fleming TP, Herlyn D, Terstappen LW, Fehm T, Tucker TF, Lane N, Wang J, Uhr JW. Circulating tumor cells in patients with breast cancer dormancy. Clin Cancer Res. 2004;10:8152–8162. - PubMed
-
- Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–1597. - PubMed
-
- Amling CL, Blute ML, Bergstralh EJ, Seay TM, Slezak J, Zincke H. Long-term hazard of progression after radical prostatectomy for clinically localized prostate cancer: continued risk of biochemical failure after 5 years. J Urol. 2000;164:101–105. - PubMed
-
- Callaway MP, Briggs JC. The incidence of late recurrence (greater than 10 years); an analysis of 536 consecutive cases of cutaneous melanoma. Br J Plast Surg. 1989;42:46–49. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
