

Poorly differentiated neuroendocrine carcinomas of the pancreas: a clinicopathologic analysis of 44 cases
- PMID: 24503751
- PMCID: PMC3977000
- DOI: 10.1097/PAS.0000000000000169
Poorly differentiated neuroendocrine carcinomas of the pancreas: a clinicopathologic analysis of 44 cases
Abstract
Background: In the pancreas, poorly differentiated neuroendocrine carcinomas include small cell carcinoma and large cell neuroendocrine carcinoma and are rare; data regarding their pathologic and clinical features are very limited.
Design: A total of 107 pancreatic resections originally diagnosed as poorly differentiated neuroendocrine carcinomas were reassessed using the classification and grading (mitotic rate/Ki67 index) criteria put forth by the World Health Organization in 2010 for the gastroenteropancreatic system. Immunohistochemical labeling for neuroendocrine and acinar differentiation markers was performed. Sixty-three cases were reclassified, mostly as well-differentiated neuroendocrine tumor (NET) or acinar cell carcinoma, and eliminated. The clinicopathologic features and survival of the remaining 44 poorly differentiated neuroendocrine carcinomas were further assessed.
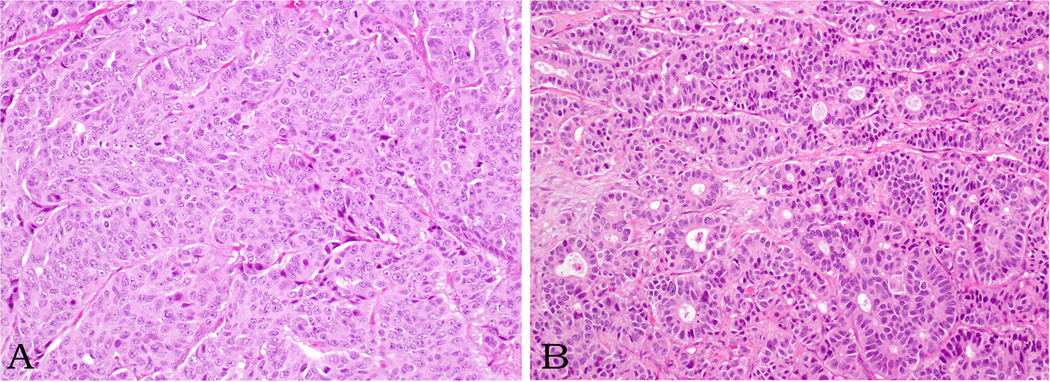
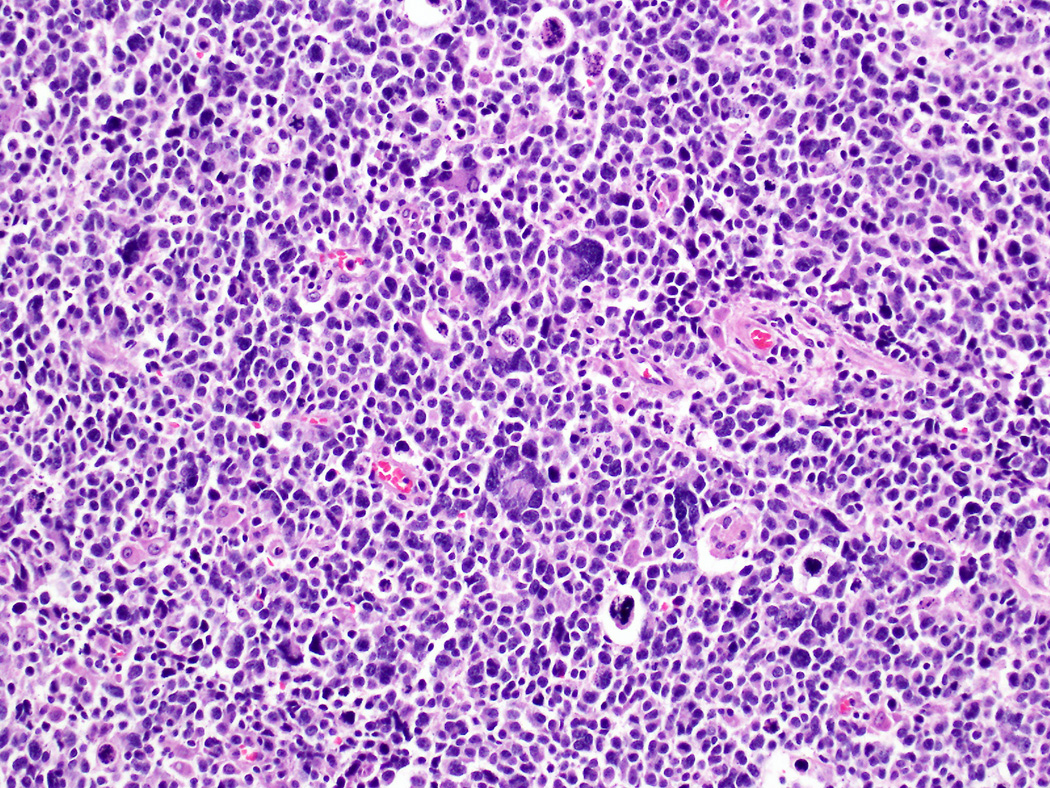
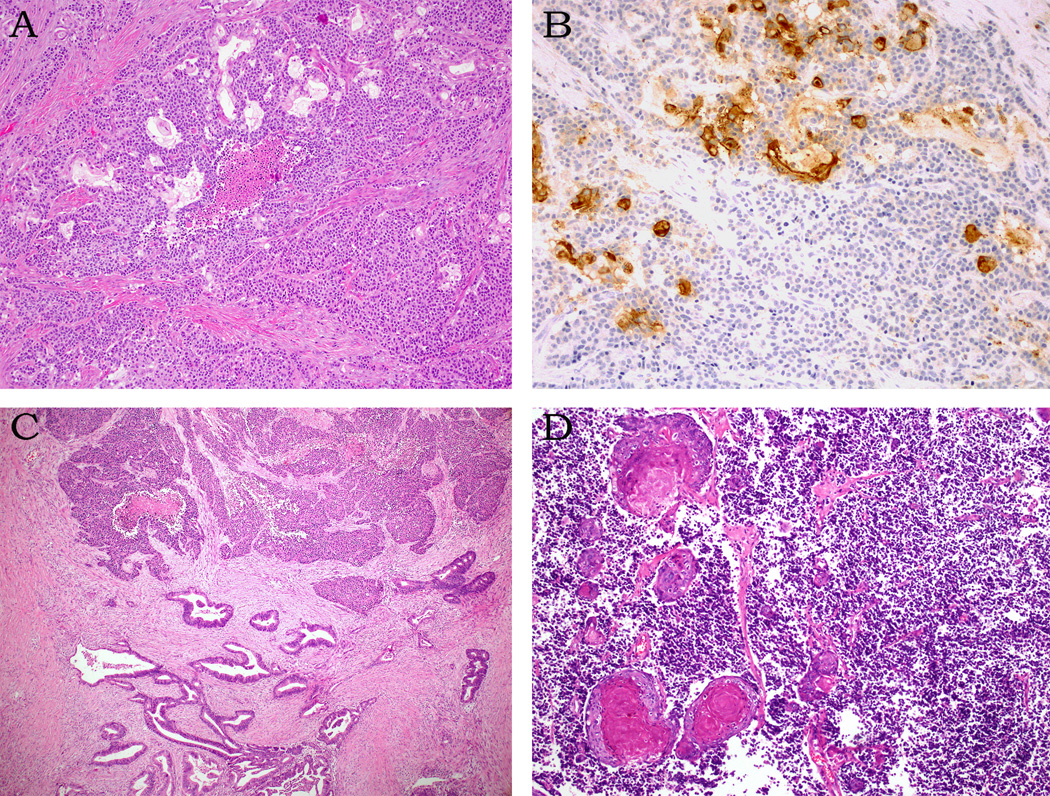
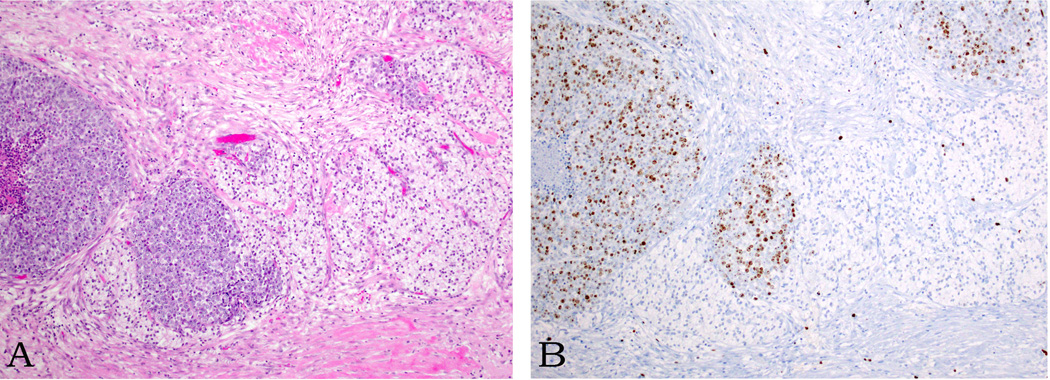
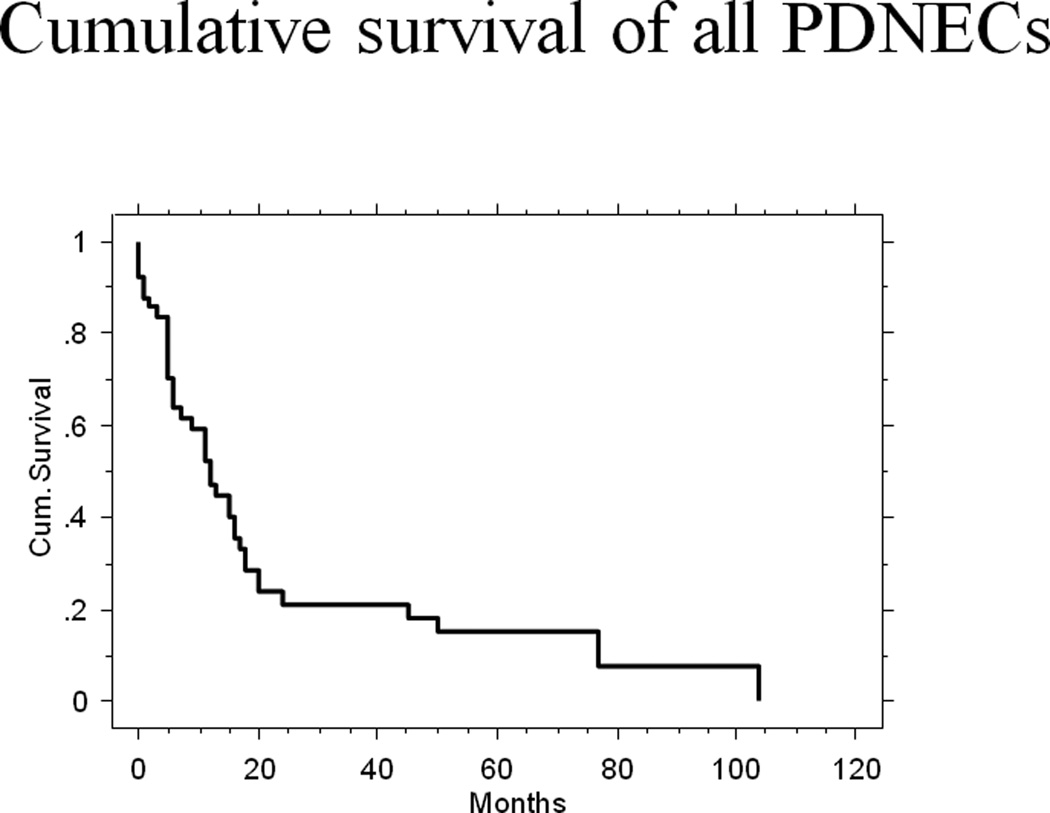
Results: The mean patient age was 59 years (range, 21 to 82 y), and the male/female ratio was 1.4. Twenty-seven tumors were located in the head of the pancreas, 3 in the body, and 11 in the tail. The median tumor size was 4 cm (range, 2 to 18 cm). Twenty-seven tumors were large cell neuroendocrine carcinomas, and 17 were small cell carcinomas (mean mitotic rate, 37/10 and 51/10 HPF; mean Ki67 index, 66% and 75%, respectively). Eight tumors had combined components, mostly adenocarcinomas. In addition, 2 tumors had components of well-differentiated NET. Eighty-eight percent of the patients had nodal or distant metastatic disease at presentation, and an additional 7% developed metastases subsequently. Follow-up information was available for 43 patients; 33 died of disease, with a median survival of 11 months (range, 0 to 104 mo); 8 were alive with disease, with a median follow-up of 19.5 months (range, 0 to 71 mo). The 2- and 5-year survival rates were 22.5% and 16.1%, respectively.
Conclusions: Poorly differentiated neuroendocrine carcinoma of the pancreas is a highly aggressive neoplasm, with frequent metastases and poor survival. Most patients die within less than a year. Most (61%) are large cell neuroendocrine carcinomas. Well-differentiated NET and acinar cell carcinoma are often misdiagnosed as poorly differentiated neuroendocrine carcinoma, emphasizing that diagnostic criteria need to be clearly followed to ensure accurate diagnosis.
Figures

References
-
- Bosman FT, et al. Neuroendocrine tumors of the GI tract. In: Bosman FT, et al., editors. WHO classification of tumors of Digestive System. Lyon: WHO Press; 2010.
-
- Bernick PE, et al. Neuroendocrine carcinomas of the colon and rectum. Dis Colon Rectum. 2004;47(2):163–169. - PubMed
-
- Brenner B, et al. Small-cell carcinomas of the gastrointestinal tract: a review. J Clin Oncol. 2004;22(13):2730–2739. - PubMed
-
- Travis WD, et al. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. World Health Organization Classification of Tumours 2004: IARC Publications - PubMed
-
- Lee SS, et al. Extrapulmonary small cell carcinoma: single center experience with 61 patients. Acta Oncol. 2007;46(6):846–851. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
