

Multimodality therapy and liver transplantation for hepatocellular carcinoma: a 14-year prospective analysis of outcomes
- PMID: 24503764
- PMCID: PMC4088318
- DOI: 10.1097/01.TP.0000441090.39840.b0
Multimodality therapy and liver transplantation for hepatocellular carcinoma: a 14-year prospective analysis of outcomes
Abstract
Background: Hepatocellular carcinoma is a major cause of death among patients with cirrhosis. A standardized approach of multimodality therapy with intent-to-treat by transplantation for all patients with hepatocellular carcinoma was instituted at our transplant center in 1997. Data were prospectively collected to evaluate the impact of multimodality therapy on posttransplant patient survival, tumor recurrence, and patient survival without transplantation.
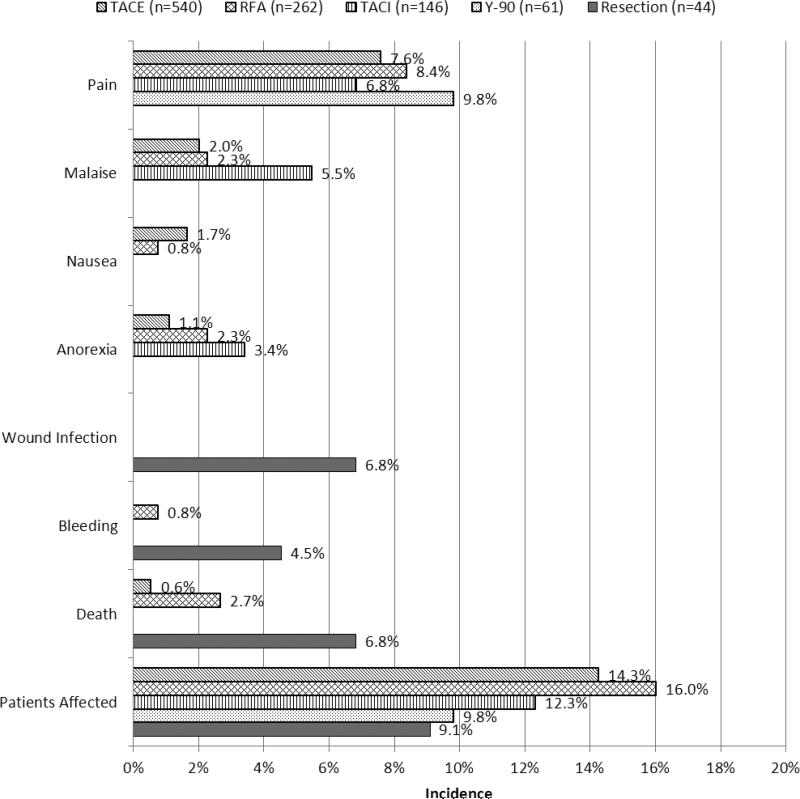
Methods: All patients with hepatocellular carcinoma were eligible for multimodality therapy. Multimodality therapy consisted of hepatic resection, radiofrequency ablation, transarterial chemoembolization, transarterial chemoinfusion, yttrium-90 microsphere radioembolization, and sorafenib.
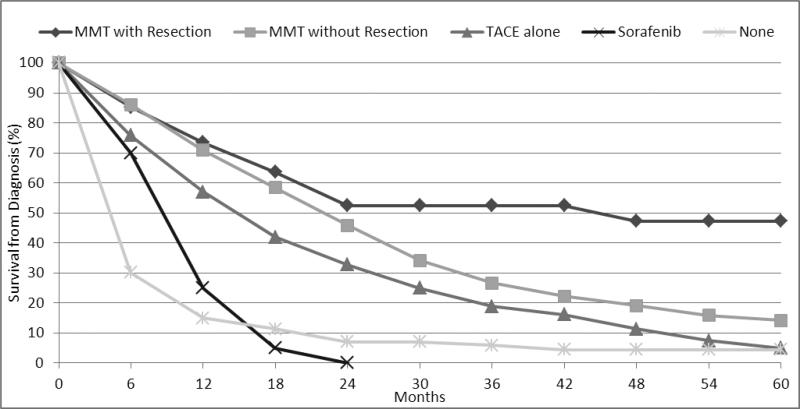
Results: Approximately 715 patients underwent multimodality therapy; 231 patients were included in the intent-to-treat with transplantation arm, and 484 patients were treated with multimodality therapy or palliative therapy because of contraindications for transplantation. A 60.2% transplantation rate was achieved in the intent-to-treat with transplantation arm. Posttransplant survivals at 1 and 5 years were 97.1% and 72.5%, respectively. Tumor recurrence rates at 1, 3, and 5 years were 2.4%, 6.2%, and 11.6%, respectively. Patients with contraindications to transplant had increased 1- and 5-year survival from diagnosis with multimodality therapy compared with those not treated (73.1% and 46.5% versus 15.5% and 4.4%, P<0.0001).
Conclusions: Using multimodality therapy before liver transplantation for hepatocellular carcinoma achieved low recurrence rates and posttransplant survival equivalent to patients with primary liver disease without hepatocellular carcinoma. Multimodality therapy may help identify patients with less active tumor biology and result in improved disease-free survival and organ utilization.
Figures
Similar articles
-
Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial.Lancet Oncol. 2015 Oct;16(13):1344-54. doi: 10.1016/S1470-2045(15)00198-9. Epub 2015 Sep 8. Lancet Oncol. 2015. PMID: 26361969 Clinical Trial.
-
Recurrent hepatocellular carcinoma in liver transplant recipients: parameters affecting time to recurrence, treatment options and survival in the sorafenib era.Tumori. 2011 Jul-Aug;97(4):436-41. doi: 10.1177/030089161109700404. Tumori. 2011. PMID: 21989430
-
Practical Considerations of Real Life of Hepatocellular Carcinoma in a Tertiary Center of Brazil.Ann Hepatol. 2017 March-April;16(2):255-262. doi: 10.5604/16652681.1231584. Ann Hepatol. 2017. PMID: 28233747
-
Management of hepatocellular carcinoma: an overview of major findings from meta-analyses.Oncotarget. 2016 Jun 7;7(23):34703-51. doi: 10.18632/oncotarget.9157. Oncotarget. 2016. PMID: 27167195 Free PMC article.
-
Management of hepatocellular carcinoma with portal vein thrombosis.World J Gastroenterol. 2015 Mar 28;21(12):3462-71. doi: 10.3748/wjg.v21.i12.3462. World J Gastroenterol. 2015. PMID: 25834310 Free PMC article. Review.
Cited by
-
Comparative Efficacy of Interventional Therapies for Early-stage Hepatocellular Carcinoma: A PRISMA-compliant Systematic Review and Network Meta-analysis.Medicine (Baltimore). 2016 Apr;95(15):e3185. doi: 10.1097/MD.0000000000003185. Medicine (Baltimore). 2016. PMID: 27082558 Free PMC article.
-
Ischemia/Reperfusion Injury and Hepatocellular Carcinoma Recurrence After Liver Transplantation: Cancer at WIT's End?Dig Dis Sci. 2015 Sep;60(9):2579-80. doi: 10.1007/s10620-015-3729-2. Dig Dis Sci. 2015. PMID: 26031422 No abstract available.
-
Treatment stage migration and treatment sequences in patients with hepatocellular carcinoma: drawbacks and opportunities.J Cancer Res Clin Oncol. 2021 Aug;147(8):2471-2481. doi: 10.1007/s00432-021-03528-3. Epub 2021 Feb 4. J Cancer Res Clin Oncol. 2021. PMID: 33537908 Free PMC article.
-
Regulatory mechanism of HIF-1α and its role in liver diseases: a narrative review.Ann Transl Med. 2022 Jan;10(2):109. doi: 10.21037/atm-21-4222. Ann Transl Med. 2022. PMID: 35282052 Free PMC article. Review.
-
Hepatocellular carcinoma: A comprehensive review.World J Hepatol. 2015 Nov 18;7(26):2648-63. doi: 10.4254/wjh.v7.i26.2648. World J Hepatol. 2015. PMID: 26609342 Free PMC article. Review.
References
-
- Di Bisceglie AM, Rustgi VK, Hoofnagle JH, Dusheiko GM, Lotze MT. NIH conference. Hepatocellular carcinoma. Ann.Intern.Med. 1988;108:390. - PubMed
-
- Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin.Liver Dis. 1999;19:329. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N.Engl.J.Med. 1996;334:693. - PubMed
-
- Halazun KJ, Verna E, Samstein B, et al. Priority pass to death - prioritization of liver transplant for HCC worsens survival. Am J Transplant. 2013;13:5, 46. - PubMed
-
- Roberts JP, Venook A, Kerlan R, Yao F. Hepatocellular carcinoma: Ablate and wait versus rapid transplantation. Liver Transpl. 2010;16:925. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
