

RET-rearranged non-small-cell lung carcinoma: a clinicopathological and molecular analysis
- PMID: 24504365
- PMCID: PMC3960615
- DOI: 10.1038/bjc.2014.36
RET-rearranged non-small-cell lung carcinoma: a clinicopathological and molecular analysis
Abstract
Background: To elucidate clinicopathological characteristics of non-small-cell lung carcinoma (NSCLC) cases carrying RET rearrangements causing oncogenic fusions to identify responders to therapy with RET tyrosine kinase inhibitors.
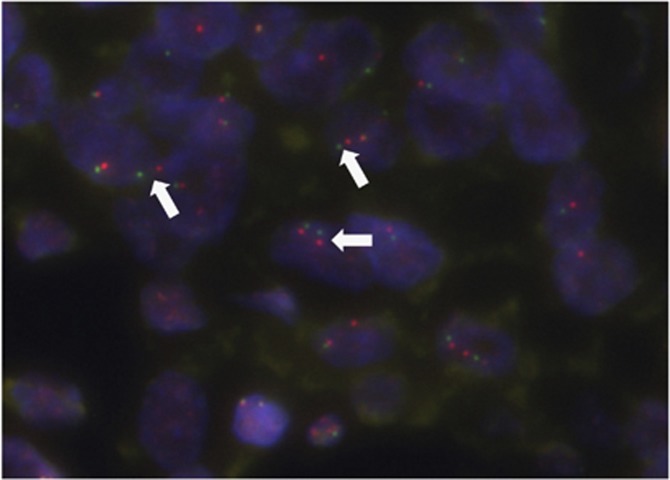
Methods: We investigated 1874 patients with carcinomas, including 1620 adenocarcinomas (ADCs), 203 squamous cell carcinomas (SCCs), 8 large cell carcinomas, and 43 sarcomatoid carcinomas (SACs). Fluorescence in situ hybridisation (FISH) and/or reverse transcription-PCR (RT-PCR) were performed to detect RET gene rearrangement.
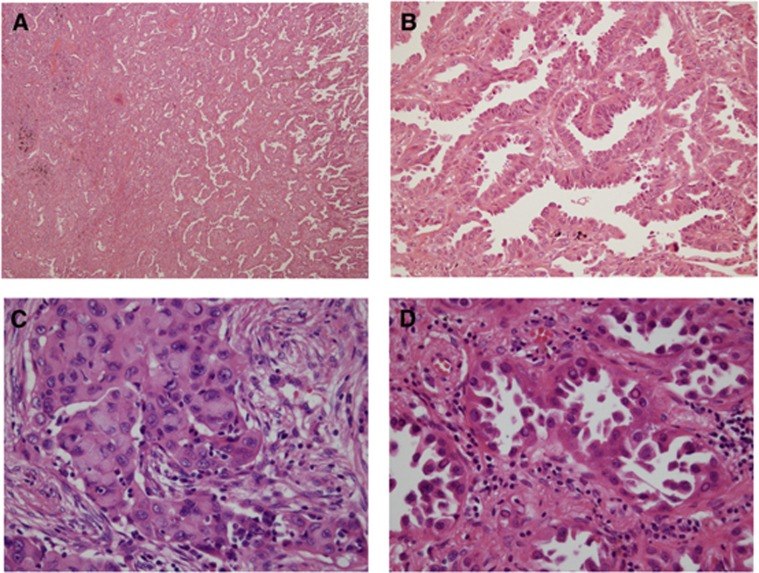
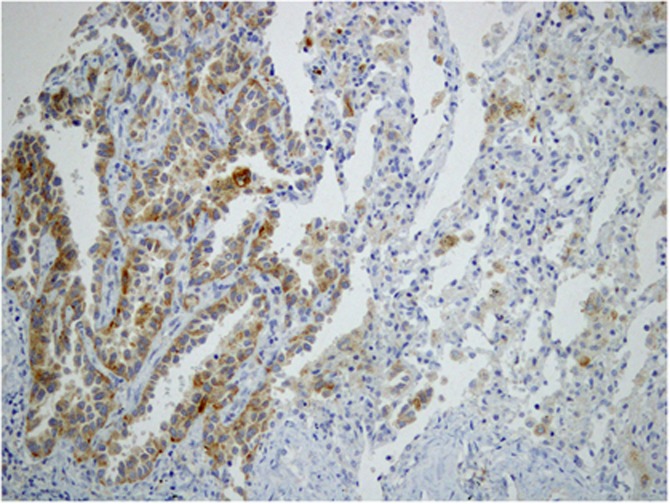
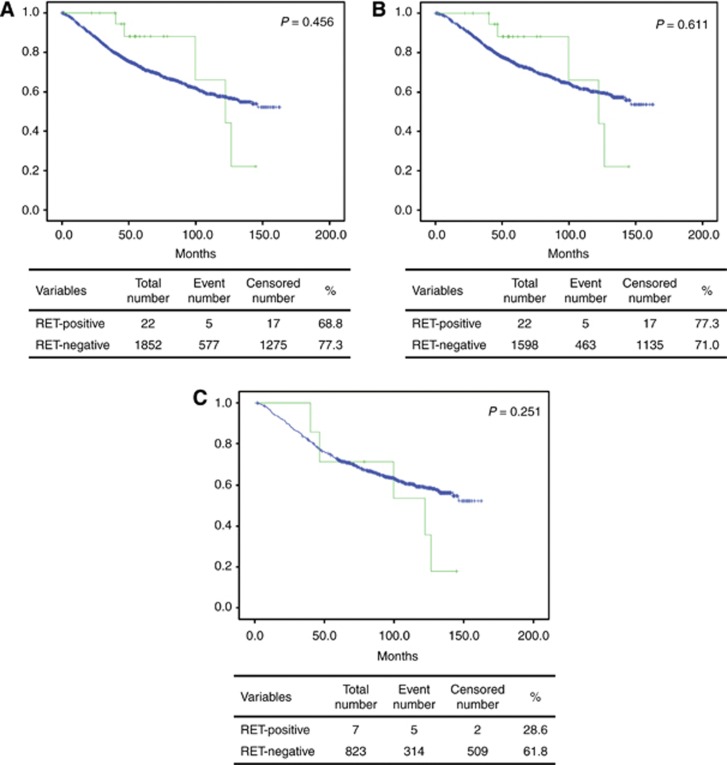
Results: In all, 22 cases (1.2%) showed RET rearrangements; all cases were of ADC histology. Of the 22 patients, 19 possessed KIF5B-RET fusion genes, whereas 3 possessed CCDC6-RET fusion genes. The RET-rearranged tumours were significantly more common in younger patients (P=0.038) and tended to occur in patients with no history of smoking (P=0.051). In addition, RET rearrangements were not associated with gender, occupational history (particularly radioactive exposure), tumour size, lymph node status, tumour stage, or patient survival. The predominant growth pattern in RET-rearranged ADCs was lepidic in 6 cases, papillary in 9 cases, acinar in 2 cases, micropapillary in 1 case, and solid in 4 cases. Cells with cytoplasmic mucin production were at least focally present in 12 of the 22 (54.5%) RET-rearranged ADC cases. Among the 21 analysed RET-rearranged tumours, RET immunopositivity was observed in 15 cases (71.4%), and was significantly associated with RET rearrangement (P<0.001).
Conclusions: The RET rearrangements were observed in 1.2% of NSCLCs. All cases of RET rearrangement were ADCs. The RET rearrangements were more likely to be observed in younger patients. Although cytoplasmic mucin production was at least focally present in 54.5% of RET-rearranged ADCs, specific histological features were not detected.
Figures
References
-
- Fukui T, Ohe Y, Tsuta K, Furuta K, Sakamoto H, Takano T, Nokihara H, Yamamoto N, Sekine I, Kunitoh H, Asamura H, Tsuchida T, Kaneko M, Kusumoto M, Yamamoto S, Yoshida T, Tamura T. Prospective study of the accuracy of EGFR mutational analysis by high-resolution melting analysis in small samples obtained from patients with non-small cell lung cancer. Clin Cancer Res. 2008;14 (15:4751–4757. - PubMed
-
- Gautschi O, Zander T, Keller FA, Strobel K, Hirschmann A, Aebi S, Diebold J. A patient with lung adenocarcinoma and RET fusion treated with vandetanib. J Thorac Oncol. 2013;8 (5:e43–e44. - PubMed
-
- Goldstraw P.2009International Association for the Study of Lung Cancer Staging Manual in Thoracic OncologyEditorial Rx Press: Florida.
-
- Grieco M, Santoro M, Berlingieri MT, Melillo RM, Donghi R, Bongarzone I, Pierotti MA, Della Porta G, Fusco A, Vecchio G. PTC is a novel rearranged form of the ret proto-oncogene and is frequently detected in vivo in human thyroid papillary carcinomas. Cell. 1990;60 (4:557–563. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
