

Differential influence of vemurafenib and dabrafenib on patients' lymphocytes despite similar clinical efficacy in melanoma
- PMID: 24504444
- PMCID: PMC4433519
- DOI: 10.1093/annonc/mdt587
Differential influence of vemurafenib and dabrafenib on patients' lymphocytes despite similar clinical efficacy in melanoma
Abstract
Background: Since the majority of melanomas eventually become resistant and progress, combining selective BRAF inhibitors (BRAFi) with immunotherapies has been proposed to achieve more durable treatment responses. Here, we explored the impact of selective BRAFi on the hosts' immune system.
Patients and methods: Clinical data, whole blood counts (WBC) and serum lactate dehydrogenase (LDH) of 277 vemurafenib- and 65 dabrafenib-treated melanoma patients were evaluated. The frequency and phenotype of lymphocyte subpopulations were determined by flow cytometry while T cell cytokine secretion was measured by multiplex assays.
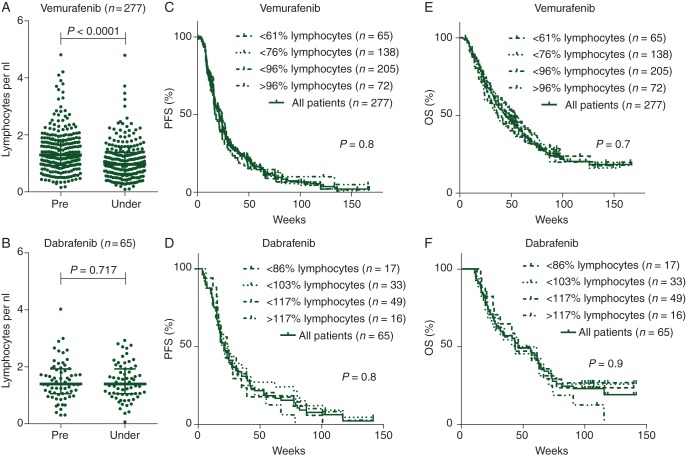
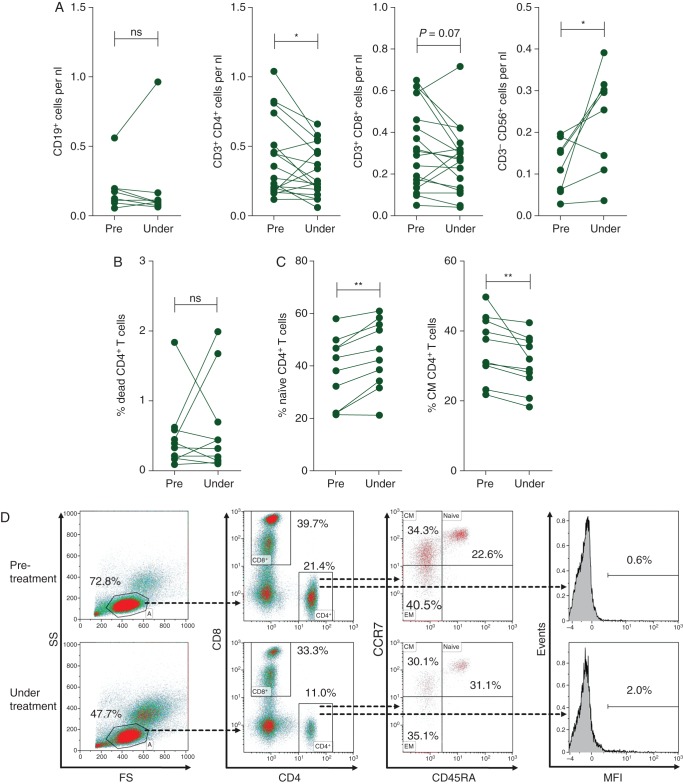
Results: Progression-free survival (PFS) as well as overall survival (OS) were similar in patients treated with either BRAFi. High pretreatment LDH was associated with shorter PFS and OS in both groups. During therapy, peripheral lymphocytes decreased by 24.3% (median, P < 0.0001) in vemurafenib-treated patients but remained unchanged in dabrafenib-treated patients (+1.2%, P = 0.717). Differentiation of peripheral lymphocytes of vemurafenib-treated patients showed a significant decrease in CD4(+) T cells (P < 0.05). Within CD4(+) T cells obtained during treatment, an increase in CCR7(+)CD45RA(+) (naïve) and a decrease in CCR7(+)CD45RA(-) (central memory) populations were found (P < 0.01 for both). Furthermore, secretion of interferon-γ and interleukin-9 by CD4(+) T cells was significantly lower in samples obtained during vemurafenib treatment compared with baseline samples.
Conclusion: While both compounds have comparable clinical efficacy, vemurafenib but not dabrafenib decreases patients peripheral lymphocyte counts and alters CD4(+) T cell phenotype and function. Thus, selective BRAFi can significantly affect patients' peripheral lymphocyte populations. Fully understanding these effects could be critical for successfully implementing combinatorial therapies of BRAFi with immunomodulatory agents.
Keywords: T cells; dabrafenib; lymphocytes; melanoma; treatment; vemurafenib.
Figures
Comment in
-
Re: Differential influence of vemurafenib and dabrafenib on patients' lymphocytes despite similar clinical efficacy in melanoma.Ann Oncol. 2014 Aug;25(8):1670-1. doi: 10.1093/annonc/mdu196. Epub 2014 Jun 1. Ann Oncol. 2014. PMID: 24890848 Free PMC article. No abstract available.
-
Reply to the letters to the editor 'Differential influence of vemurafenib and dabrafenib on patients' lymphocytes despite similar clinical efficacy in melanoma' by Diwakar et al.Ann Oncol. 2015 Jan;26(1):250-251. doi: 10.1093/annonc/mdu502. Epub 2014 Oct 29. Ann Oncol. 2015. PMID: 25355721 No abstract available.
References
-
- Jang S, Atkins MB. Which drug, and when, for patients with BRAF-mutant melanoma? Lancet Oncol. 2013;14:e60–e69. - PubMed
-
- Boni A, Cogdill AP, Dang P, et al. Selective BRAFV600E inhibition enhances T cell recognition of melanoma without affecting lymphocyte function. Cancer Res. 2010;70:5213–5219. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
