

Effect of an educational toolkit on quality of care: a pragmatic cluster randomized trial
- PMID: 24505216
- PMCID: PMC3913553
- DOI: 10.1371/journal.pmed.1001588
Effect of an educational toolkit on quality of care: a pragmatic cluster randomized trial
Abstract
Background: Printed educational materials for clinician education are one of the most commonly used approaches for quality improvement. The objective of this pragmatic cluster randomized trial was to evaluate the effectiveness of an educational toolkit focusing on cardiovascular disease screening and risk reduction in people with diabetes.
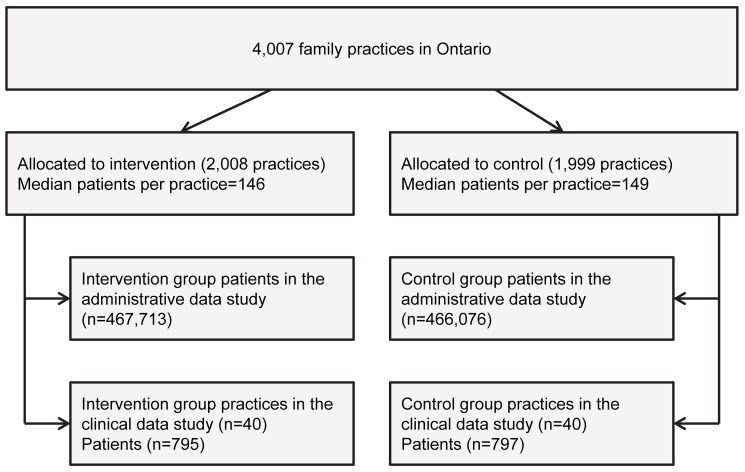
Methods and findings: All 933,789 people aged ≥40 years with diagnosed diabetes in Ontario, Canada were studied using population-level administrative databases, with additional clinical outcome data collected from a random sample of 1,592 high risk patients. Family practices were randomly assigned to receive the educational toolkit in June 2009 (intervention group) or May 2010 (control group). The primary outcome in the administrative data study, death or non-fatal myocardial infarction, occurred in 11,736 (2.5%) patients in the intervention group and 11,536 (2.5%) in the control group (p = 0.77). The primary outcome in the clinical data study, use of a statin, occurred in 700 (88.1%) patients in the intervention group and 725 (90.1%) in the control group (p = 0.26). Pre-specified secondary outcomes, including other clinical events, processes of care, and measures of risk factor control, were also not improved by the intervention. A limitation is the high baseline rate of statin prescribing in this population.
Conclusions: The educational toolkit did not improve quality of care or cardiovascular outcomes in a population with diabetes. Despite being relatively easy and inexpensive to implement, printed educational materials were not effective. The study highlights the need for a rigorous and scientifically based approach to the development, dissemination, and evaluation of quality improvement interventions.
Trial registration: http://www.ClinicalTrials.gov NCT01411865 and NCT01026688.
Conflict of interest statement
BRS was a member of the Guideline Dissemination and Implementation Committee and the National Research Council of the Canadian Diabetes Association (CDA) at the time of the study. OB was a member of the Executive of the Clinical and Scientific Section and the Guideline Dissemination and Implementation Committee of the CDA at the time of the study. CHYY is currently Chair of the Guideline Dissemination and Implementation Committee of the CDA. MMM has served as an Advisory Board member for the following pharmaceutical companies: Astra Zeneca, Bristol-Myers Squibb, Eli Lilly and Company, Glaxo Smith Kline, Hoffman La Roche, Novartis, Novo Nordisk, and Pfizer. JAP has served as both a guest academic editor and a reviewer for
Figures
References
-
- Stewart AL, Greenfield S, Hays RD, Wells K, Rogers WH, et al. (1989) Functional status and well-being of patients with chronic conditions. Results from the Medical Outcomes Study. JAMA 262: 907–913. - PubMed
-
- Gregg EW, Gu Q, Cheng YJ, Narayan KMV, Cowie CC (2007) Mortality trends in men and women with diabetes, 1971 to 2000. Ann Intern Med 147: 149–155. - PubMed
-
- Dawson KG, Gomes D, Gerstein H, Blanchard JF, Kahler KH (2002) The economic cost of diabetes in Canada, 1998. Diabetes Care 25: 1303–1307. - PubMed
-
- Canadian Diabetes Association Clinical Practice Guidelines Expert Committee (2008) Canadian Diabetes Association 2008 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes 32: S1–S201. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
