

Positive network assortativity of influenza vaccination at a high school: implications for outbreak risk and herd immunity
- PMID: 24505274
- PMCID: PMC3914803
- DOI: 10.1371/journal.pone.0087042
Positive network assortativity of influenza vaccination at a high school: implications for outbreak risk and herd immunity
Abstract
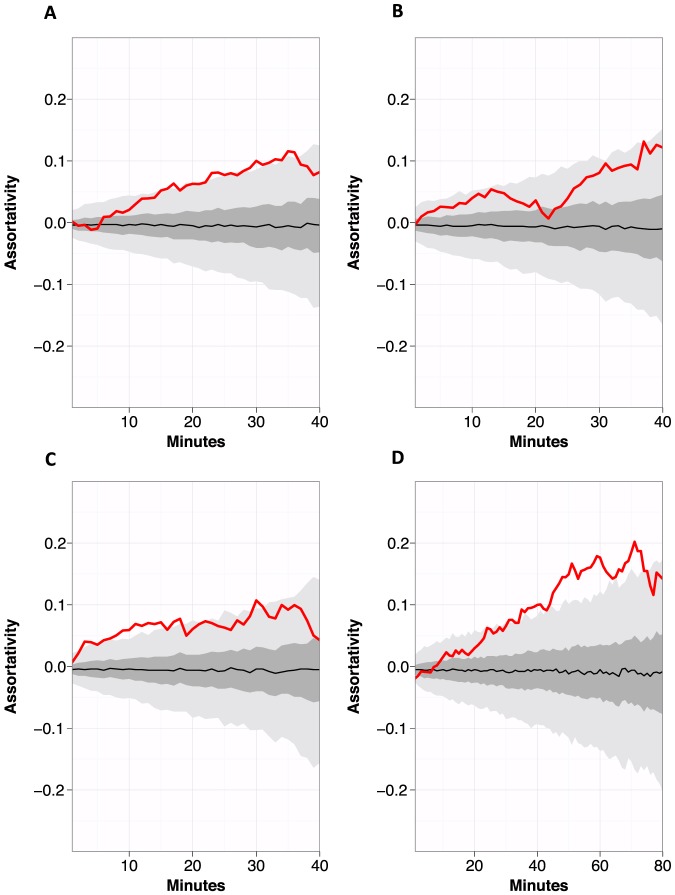
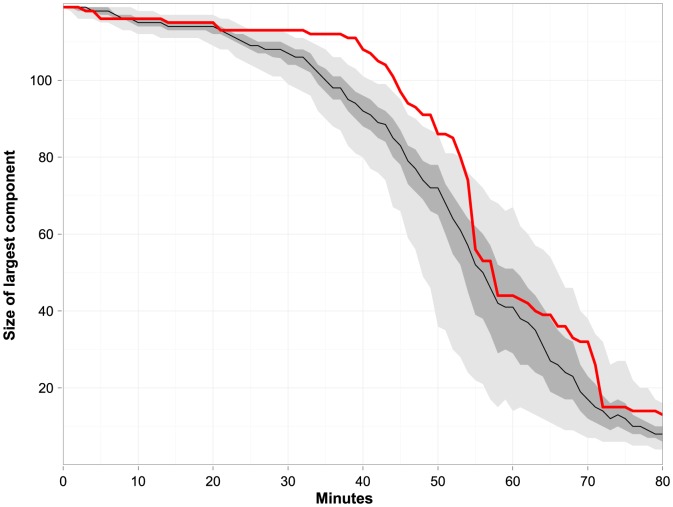
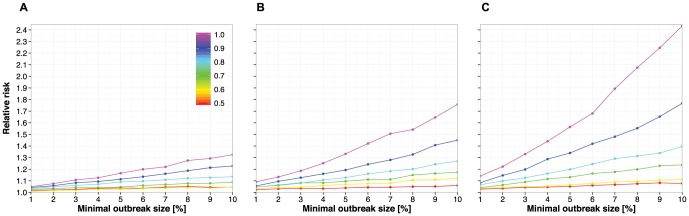
Schools are known to play a significant role in the spread of influenza. High vaccination coverage can reduce infectious disease spread within schools and the wider community through vaccine-induced immunity in vaccinated individuals and through the indirect effects afforded by herd immunity. In general, herd immunity is greatest when vaccination coverage is highest, but clusters of unvaccinated individuals can reduce herd immunity. Here, we empirically assess the extent of such clustering by measuring whether vaccinated individuals are randomly distributed or demonstrate positive assortativity across a United States high school contact network. Using computational models based on these empirical measurements, we further assess the impact of assortativity on influenza disease dynamics. We found that the contact network was positively assortative with respect to influenza vaccination: unvaccinated individuals tended to be in contact more often with other unvaccinated individuals than with vaccinated individuals, and these effects were most pronounced when we analyzed contact data collected over multiple days. Of note, unvaccinated males contributed substantially more than unvaccinated females towards the measured positive vaccination assortativity. Influenza simulation models using a positively assortative network resulted in larger average outbreak size, and outbreaks were more likely, compared to an otherwise identical network where vaccinated individuals were not clustered. These findings highlight the importance of understanding and addressing heterogeneities in seasonal influenza vaccine uptake for prevention of large, protracted school-based outbreaks of influenza, in addition to continued efforts to increase overall vaccine coverage.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
