

What is the evidence for physical therapy poststroke? A systematic review and meta-analysis
- PMID: 24505342
- PMCID: PMC3913786
- DOI: 10.1371/journal.pone.0087987
What is the evidence for physical therapy poststroke? A systematic review and meta-analysis
Abstract
Background: Physical therapy (PT) is one of the key disciplines in interdisciplinary stroke rehabilitation. The aim of this systematic review was to provide an update of the evidence for stroke rehabilitation interventions in the domain of PT.
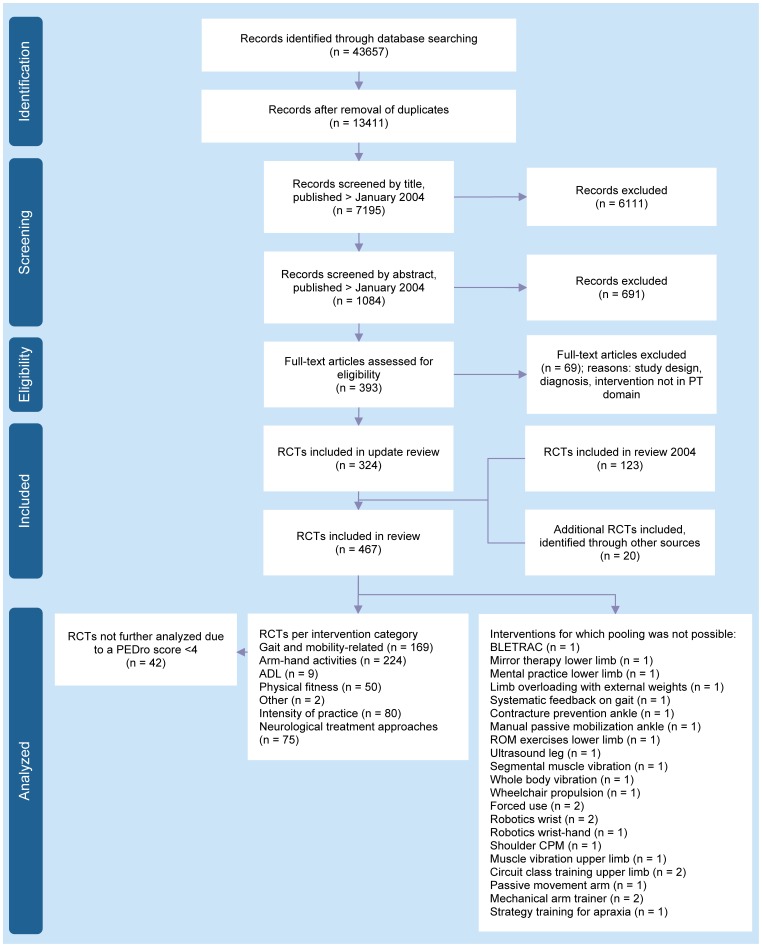
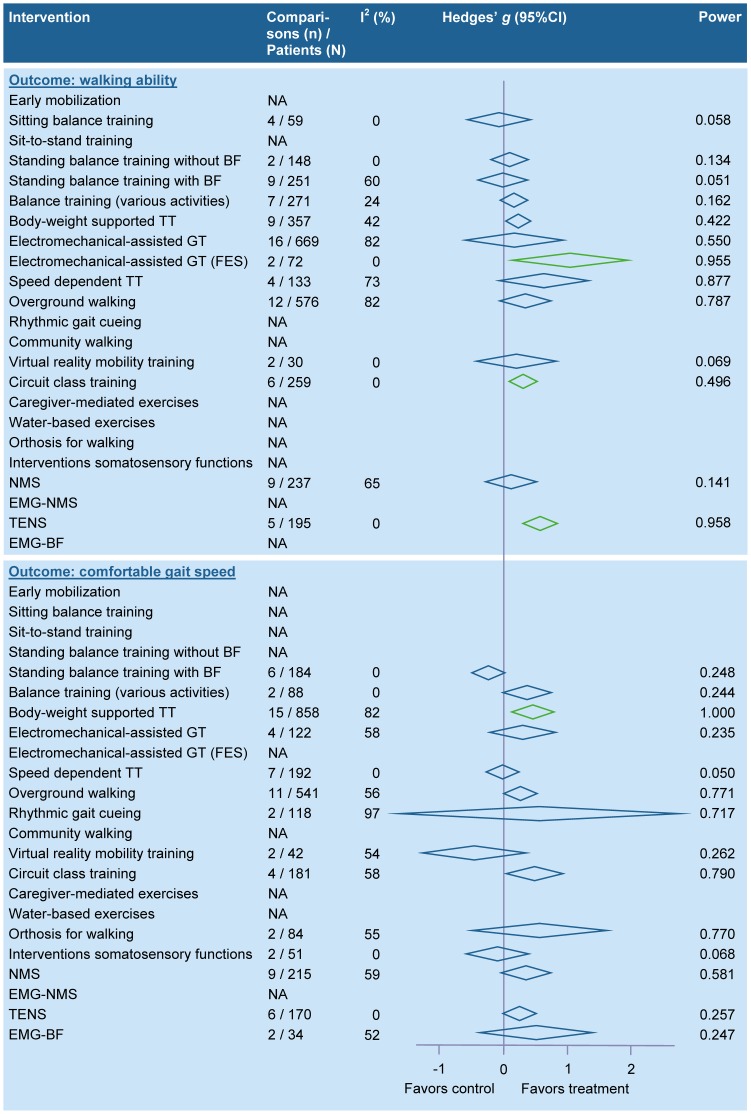
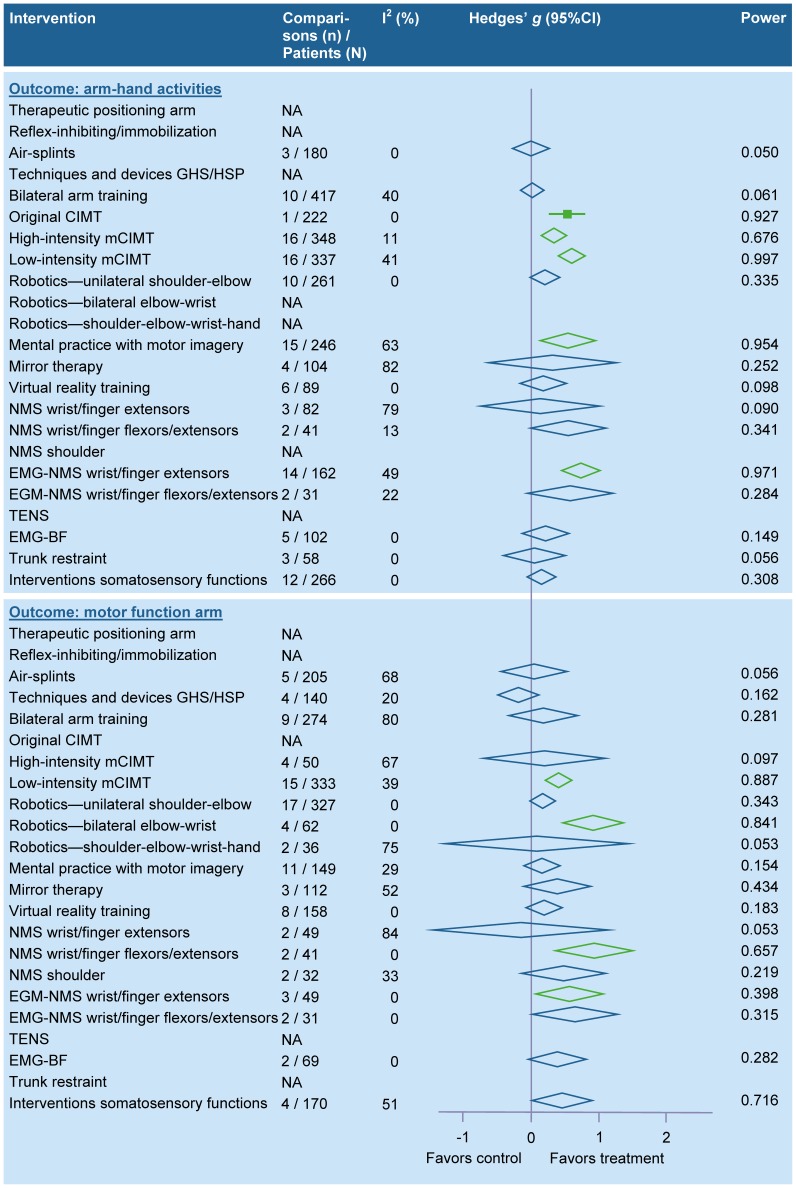
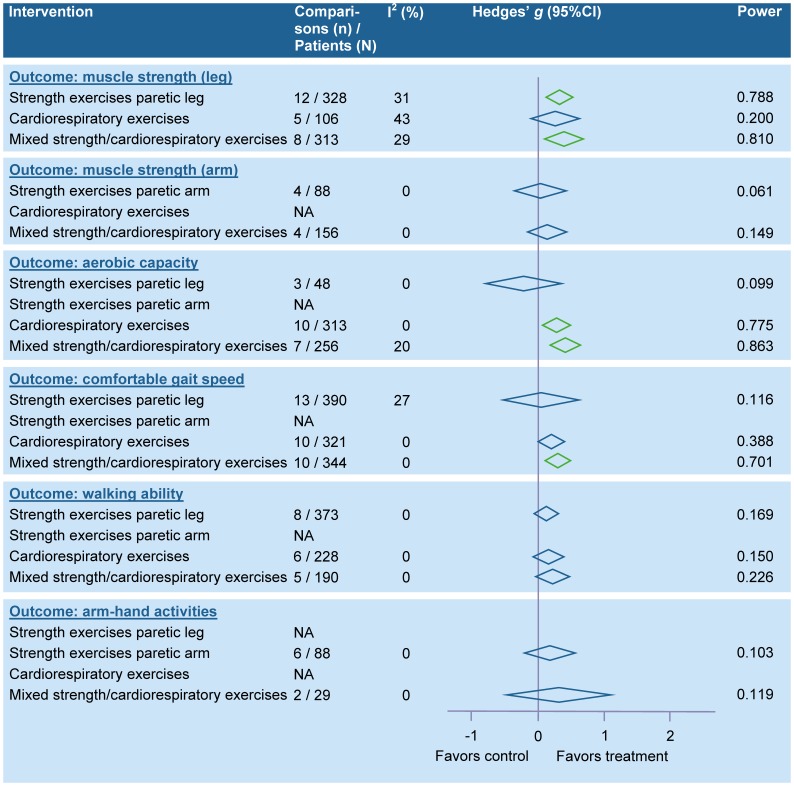
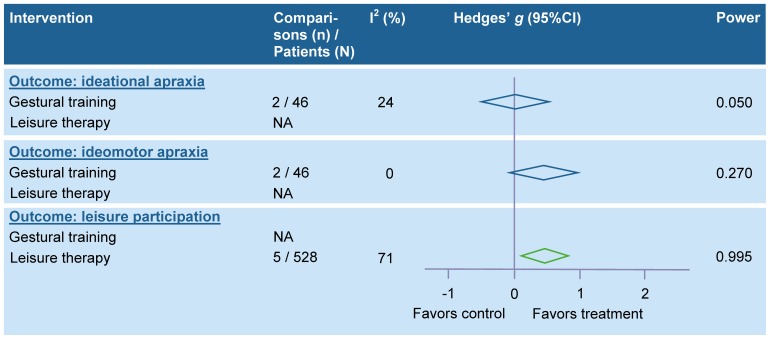
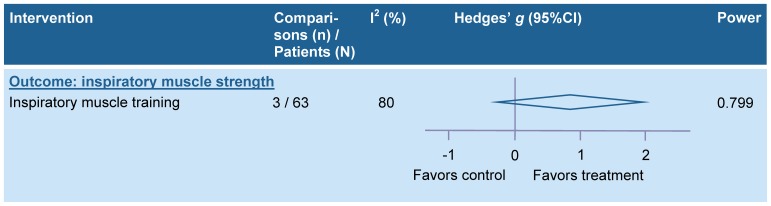
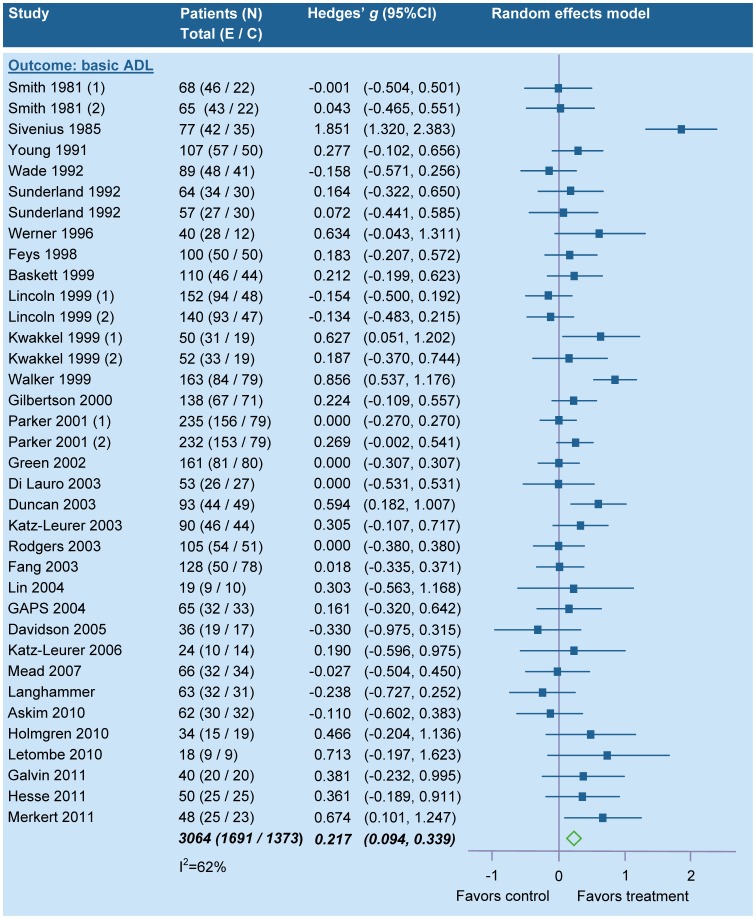
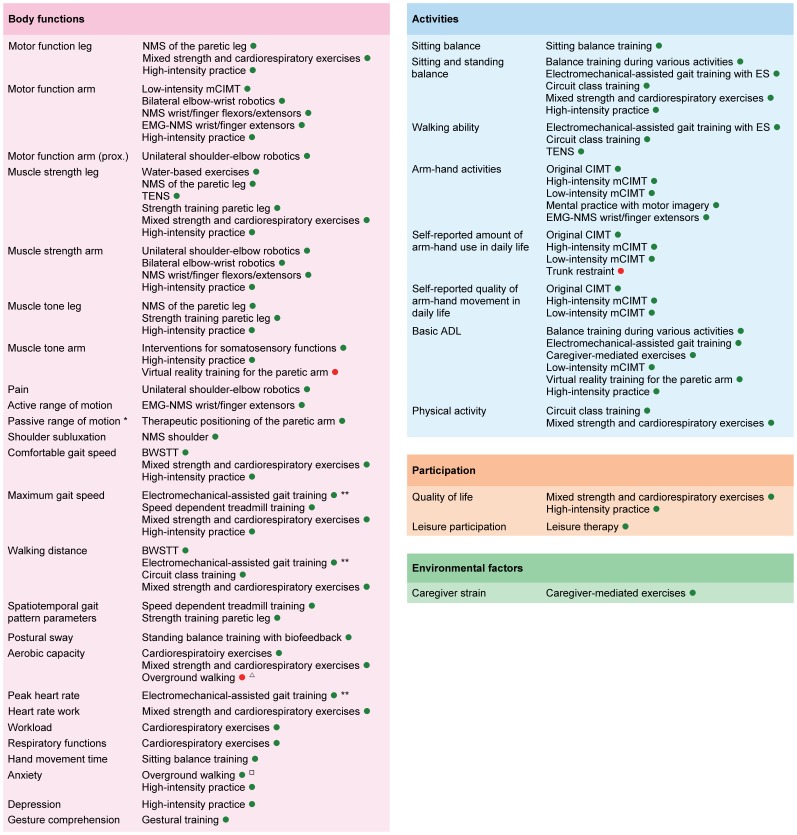
Methods and findings: Randomized controlled trials (RCTs) regarding PT in stroke rehabilitation were retrieved through a systematic search. Outcomes were classified according to the ICF. RCTs with a low risk of bias were quantitatively analyzed. Differences between phases poststroke were explored in subgroup analyses. A best evidence synthesis was performed for neurological treatment approaches. The search yielded 467 RCTs (N = 25373; median PEDro score 6 [IQR 5-7]), identifying 53 interventions. No adverse events were reported. Strong evidence was found for significant positive effects of 13 interventions related to gait, 11 interventions related to arm-hand activities, 1 intervention for ADL, and 3 interventions for physical fitness. Summary Effect Sizes (SESs) ranged from 0.17 (95%CI 0.03-0.70; I(2) = 0%) for therapeutic positioning of the paretic arm to 2.47 (95%CI 0.84-4.11; I(2) = 77%) for training of sitting balance. There is strong evidence that a higher dose of practice is better, with SESs ranging from 0.21 (95%CI 0.02-0.39; I(2) = 6%) for motor function of the paretic arm to 0.61 (95%CI 0.41-0.82; I(2) = 41%) for muscle strength of the paretic leg. Subgroup analyses yielded significant differences with respect to timing poststroke for 10 interventions. Neurological treatment approaches to training of body functions and activities showed equal or unfavorable effects when compared to other training interventions. Main limitations of the present review are not using individual patient data for meta-analyses and absence of correction for multiple testing.
Conclusions: There is strong evidence for PT interventions favoring intensive high repetitive task-oriented and task-specific training in all phases poststroke. Effects are mostly restricted to the actually trained functions and activities. Suggestions for prioritizing PT stroke research are given.
Conflict of interest statement
Figures
References
-
- Wardlaw J, Murray V, Berge E, Del Zoppo G (2009) Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev: CD000213. - PubMed
-
- Stroke Unit Trialists' Collaboration (2007) Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev: CD000197. - PubMed
-
- Miller E, Murray L, Richards L, Zorowitz R, Bakas T, et al. (2010) Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke patient: a scientific statement from the American Heart Association. Stroke 41: 2402–2448. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
