

Are we doing enough to stem the tide of acquired MDR-TB in countries with high TB burden? Results of a mixed method study in Chongqing, China
- PMID: 24505476
- PMCID: PMC3914979
- DOI: 10.1371/journal.pone.0088330
Are we doing enough to stem the tide of acquired MDR-TB in countries with high TB burden? Results of a mixed method study in Chongqing, China
Abstract
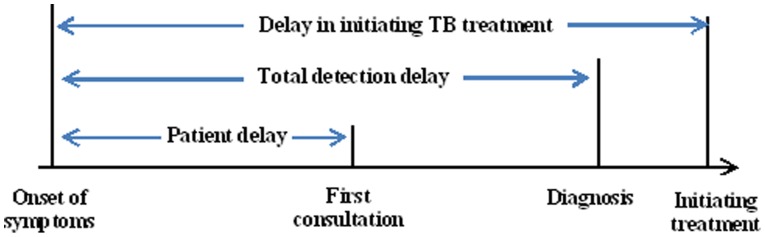
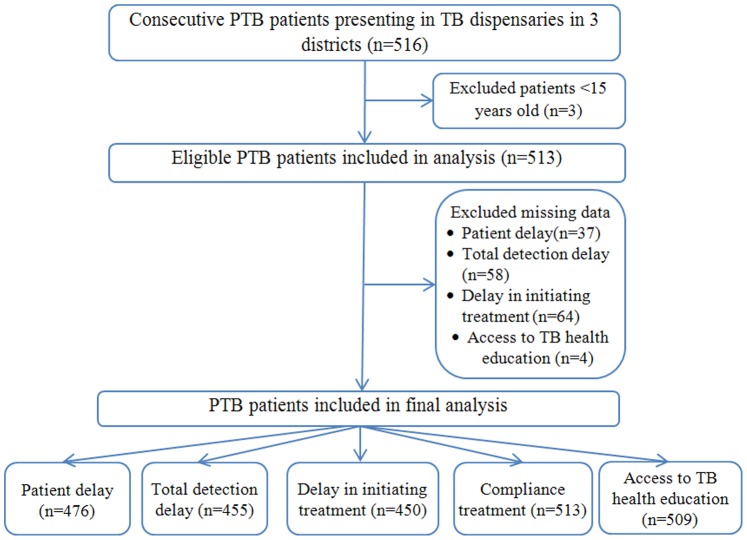
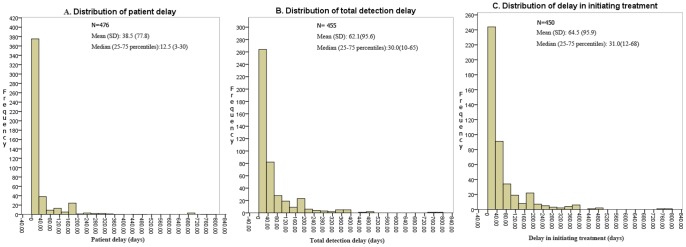
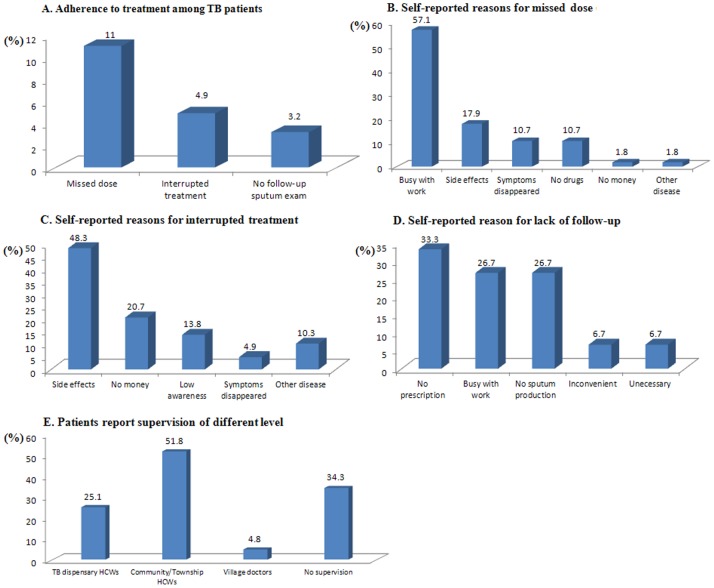
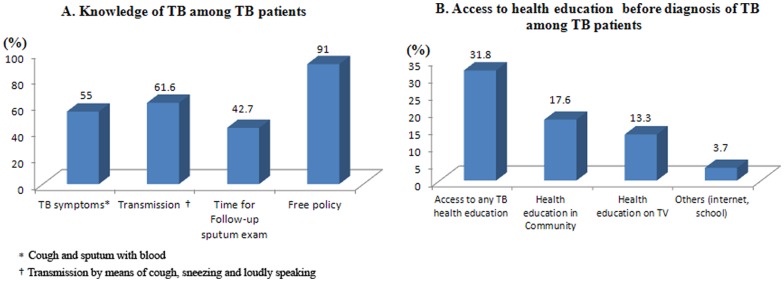
Multi-drug resistant tuberculosis (MDR-TB) represents a threat to health and development in countries with high TB burden. China's MDR-TB prevalence rate of 6.8% is the highest in the world. Interventions to remove barriers against effective TB control, and prevention of MDR-TB are urgently needed in the country. This paper reports a cross-sectional questionnaire survey of 513 pulmonary TB (PTB) patients, and qualitative interviews of 10 healthcare workers (HCWs), and 15 PTB patients. The objective was to assess barriers against effective control of PTB and prevention of MDR-TB by elucidating the perspectives of patients and healthcare providers. Results showed that more than half of the patients experienced patient delay of over 12.5 days. A similar proportion also experienced detection delay of over 30 days, and delay in initiating treatment of over 31 days. Consulting a non-TB health facility ≥3 times before seeking care at TB dispensary was a risk factor for both detection delay [AOR (95% CI): 1.89(1.07, 3.34) and delay in initiating treatment[AOR (95% CI): 1.88 (1.06, 3.36). Results revealed poor implementation of Directly Observed Therapy (DOT), whereby treatment of 34.3% patients was never monitored by HCWs. Only 31.8% patients had ever accessed TB health education before their TB diagnosis. Qualitative data consistently disclosed long patient delay, and indicated that patient's poor TB knowledge and socioeconomic barriers were primary reasons for patient delay. Seeking care and being treated at a non-TB hospital was an important reason for detection delay. Patient's long work hours and low income increased risk for treatment non-adherence. Evidence-based measures to improve TB health seeking behavior, reduce patient and detection delays, improve the quality of DOT, address financial and system barriers, and increase access to TB health promotion are urgently needed to address the burgeoning prevalence of MDR-TB in China.
Conflict of interest statement
Figures
References
-
- WHO: Global tuberculosis report 2012. Available: http://apps.who.int/iris/bitstream/10665/75938/1/9789241564502_eng.pdf. Accessed 2013 July 28.
-
- Ormerod LP (2005) Multidrug-resistant tuberculosis (MDR-TB): epidemiology, prevention and treatment. Br Med Bull 73–74: 17–24. - PubMed
-
- Pablos-Méndez A, Raviglione MC, Laszlo A, Binkin N, Rieder HL, et al. (1998) Global surveillance for anti-tuberculosis drug resistance 1994–1997. World Health Organization–International Union Against Tuberculosis and Lung Disease Working Group on Anti Tuberculosis Drug Resistance Surveillance. N Engl J Med 338: 1641–9. - PubMed
-
- Abubakar I, Zignol M, Falzon D, Raviglione M, Ditiu L, et al. (2013) Drug-resistant tuberculosis: time for visionary political leadership. Lancet Infect Dis 13: 529–39. - PubMed
-
- Fitzpatrick C, Floyd K (2012) A systematic review of the cost and cost effectiveness of treatment for multidrug-resistant tuberculosis. Pharmacoeconomics 30: 63–80. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
